



Nazi Healthcare Revived Across the Five Eyes: Killing Useless Eaters and Biden’s COVID Relief Bill
March 12, 2021
“The ill-conceived `love of thy neighbor’ has to disappear, especially in relation to inferior or asocial creatures. It is the supreme duty of a national state to grant life and livelihood only to the healthy and hereditarily sound portion of the people in order to secure the maintenance of a hereditarily sound and racially pure folk for all eternity….”
-Dr. Arthur Guett, Nazi Director of Public Health, 1935
The words spoken by Dr. Guett 85 years ago should send shivers down the spine of anyone following the radical transformations of healthcare policy now underway within the Five Eyes zone of influence.
As many people are now aware, embedded within the $1.9 trillion COVID relief package is a $40 billion program to revive and expand the corpse of Obama Care’s enrollment protocols and the worst aspects of State directed medical resource allocation for the most vulnerable (and financially burdensome) of society. While few details have been unveiled beyond a mass expansion of enrollment into the plan on a revived healthcare.gov, several red alarms have been raised which began with the appointment of Obama-care architect Ezekiel Emmanuel to Biden’s COVID task force last year and the re-ascendency of hives of cost-cutting behaviorists to positions of power.
 Modernity Without Rest...
Check Amazon for Pricing.
Modernity Without Rest...
Check Amazon for Pricing.

Before I proceed, a small disclaimer is in order.
Just because I am about to viciously criticize Biden/Obama-care, and the accelerated expansion of euthanasia across Five Eyes nations, it does NOT mean that I support free-market “greed-is-good” HMOs that were brought online by Nixon in 1973.
As I wrote in my recent trilogy exposing the contrived debates between “statist” Malthusian John Maynard Keynes vs “individualist” Malthusian Friedrich von Hayek, the schism of top down vs bottom up economic thinking which has brainwashed several generations of Americans is a chimera with no bearing in reality. Real economics that befits human life and dignity has always defended the whole of society while also protecting the unalienable rights and liberty of each individual within society.
If you are a technocrat looking down upon the world from your ivory mathematical tower at the impending crises hitting civilization, you would not believe a word of what I just said. Rather you would be looking at a glaring “mathematical disequilibrium” rushing towards us like a tsunami: The western population concentrated in the Trans Atlantic nations is facing a demographic time bomb the likes of which has never been seen in history called by some “the babyboomer demographic time bomb”.
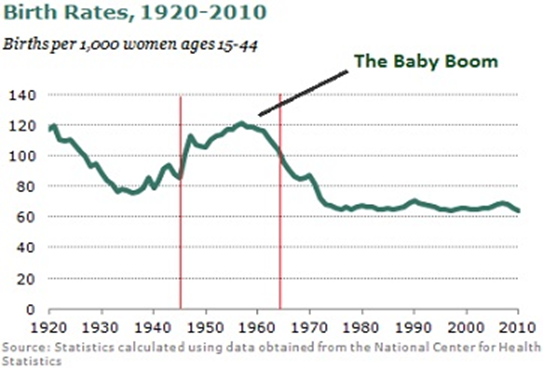
Even before COVID-19 annihilated much of the world economy, the baby boomer demographic time bomb was discussed by think tanks and policy makers far and wide. During the past 25 years, young people increasingly put off having children (with a 4.4% collapse in birthrates during the Dec. 2019-Dec 2020 year of COVID). Today western fertility levels have fallen to 1.7 children/woman which is far below the 2.1 levels needed to replace the population.
During this time, the baby boomer generation born between 1945-1960 increasingly found themselves beset with grey hair, and increased healthcare needs in their old age with the first wave having hit retirement years in 2010. While technological advances has extended average life expectancies from 61 years (in 1935) to 81 years today, the demographic imbalance of young : old means that society will essentially be incapable of supporting itself under current dynamics.
For example:
By 2030, it is currently estimated people over the age of 85 will triple while seniors between 65-85 will double. The financial costs of sustaining this demographic will skyrocket as healthcare services double from their currently massive $1.4 trillion/year to $3 trillion/year by 2050 (in the USA).
As cost-effectiveness experts look at this dismal trend, all they can see is a cold numbers game.
These experts don’t tend to see humans with cognitive powers and souls and they certainly don’t recognize the existence of such immaterial notions as the “sacred” which might prevent the culling of lives in order to satisfy monetary constraints.
They certainly don’t recognize the injustices of a system that allows trillions of dollars to be spent for Wall Street bailouts and Middle East wars but which fails to provide the medical resources to service its own population fairly. The experts I am talking about who once ruled America under Barack Obama and who have resurged into power under Biden only see the cold fact that 80% or more of the healthcare costs absorbed throughout one’s life occur after 65 years of age. These experts can only think in terms of adapting to scarcity and supposedly “fixed limits” but never eliminating scarcity through systemic changes that place human life and creative thought on a higher priority than mere money.
 History of Political I...
Check Amazon for Pricing.
History of Political I...
Check Amazon for Pricing.
With ever fewer young people entering the work force (and with the financial system itself set to meltdown under hyperinflation), two options present themselves:
- Recognize that the system is broken and transform it in such a way that national spending priorities are re-directed towards large-scale, long term infrastructure building and cooperation with other nations among the multipolar alliance
OR
- Work within the rules of the broken system and cull the human herd to diminish costs associated with “scarce medical resources”.
The Genocidal Mind of Dr. Ezekiel Emmanuel
As it stands, the individual most responsible for reviving Obamacare and the associated “Independent Payment Advisory Board” (IPAB) of cost-effectiveness “experts” under Joe Biden is the same figure who crafted the original Affordable Care Act (aka: Obamacare) in 2009. While acting as Obama’s health advisor from 2009-2011, Ezekiel Emmanuel wrote a bone chilling study called “Principles for allocation of scarce medical interventions” in the Lancet. In this revealing document, Ezekiel’s vision for a new ethic of healthcare management was enunciated with the “Complete Lives System” that would be used to justify who among the needy of society competing for scraps of the shrinking pie, will receive care (i.e: expensive cancer screenings, treatments, drugs), and who will be left to die when he wrote:
“When implemented, the complete lives system produces a priority curve on which individuals aged between roughly 15 to 40 years gets the most substantial chances, whereas the youngest and the oldest people get chances that are attenuated.”
Overthrowing the entire edifice of Judeo-Christian values that defined human life as sacred as well as the pesky Hippocratic oath which prevents physicians from doing any harm willfully to their patients, Emmanuel describes exactly what he intends by his “priority curve” and “attenuated chances” for the young and old saying:
“Strict youngest-first allocation directs scarce resources predominantly to infants. This approach seems incorrect. The death of a 20-year-old woman is intuitively worse than that of a 2-month-old girl, even though the baby has had less life. The 20 year old has a much more developed personality than the infant, and has drawn upon the investment of others to begin as yet-unfulfilled projects… adolescents have received substantial education and parental care, investment that will be wasted without a complete life: infants by contrast, have not yet received these investments… it is terrible when an infant dies, but worse, most people think, when a three year old child dies, and worse still when an adolescent dies.”

That’s right: Emmanuel’s “cost-effective” curve asserts that the life of a 20-year-old is more worthy of life than that of a 3-year-old, or 75 year old. In the latter two cases, society has invested either too little to make that young life worth saving or has invested too much already (relative to the financial worth of the low QALY senior).
In a more recent 2014 article published in the Atlantic, called ‘Why I Hope to Die at 75’, Emmanuel explained his belief that anyone attempting to prolong their life beyond 75 is delusional, selfish and pathetic stating: “I think this manic desperation to endlessly extend life is misguided and potentially destructive. For many reasons, 75 is a pretty good age to aim to stop.”
When Obama came to power in 2008, many were confused with his decision to destroy any actual proposals for universal health coverage for which he had apparently campaigned (such as Rep. John Conyers single-payer Bill H.R. 676). Instead of supporting Conyer’s bill, Obama and his hive of Economic Behaviorists only amplified the power of the private HMOs by forcing citizens to purchase coverage while infusing billions of tax payer funds into private insurers.
The reason was simple: Conyers’ bill didn’t mandate cuts to healthcare spending, but rather amplified spending for health services while providing healthcare to all Americans with no strings attached. Obama’s controllers had other ideas, as the former president stated in 2010:
“We believe the reforms we’ve proposed to strengthen Medicare and Medicaid will enable us to keep these commitments to our citizens while saving us $500 billion by 2023, and an additional $1 trillion in the decade after that.”
A paradox arises: How was Obama planning to extend medical coverage to the 27 million uninsured while cutting $1 trillion in health expenditures over a decade?
Quality Adjusted Life Years and Death Panels
Ezekiel Emmanuel made the point in his 2009 report that the key to cost cutting in health care would be found in the application of Quality Adjusted Life Years (QALYs) under the control of independent panels of experts. The QALY system was itself pioneered under Britain’s National Institute of Clinical Excellence (NICE) and Liverpool Care Pathway System which were driving forces behind the corruption of Britain’s National Healthcare System (NHS) from 1999-present. The former head of NICE (Sir Michael Rawlins) defined QALYs in the following terms in a March 2009 interview with Time Magazine:
“It’s based on the cost of a measure called the ‘quality-adjusted life year.’ A QALY scores your health on a scale from zero to one: zero if you’re dead and one if you’re in perfect health. You find out as a result of a treatment where a patient would move up the scale. If you do a hip replacement, the patient might start at 0.5 and go up to 0.7, improving 0.2. You can assume patients live for an average of 15 years following hip replacements. And .2 times 15 equals three quality adjusted life years. If the hip replacement costs £10,000 to do, it’s 10,000 divided by three, which equals £3,333. That figure is the cost per QALY.”
Another co-architect of Obamacare alongside Emmanuel was a fellow named Sir Donald Berwick (knighted in 2005) who stated candidly that “the decision is not whether or not we will ration care- the decision is whether we will ration with our eyes open.”
Another key behaviorist assigned to create Obamacare was MIT professor Jonathan Gruber who created a scandal when he admitted on camera to using obscurantist language and secrecy when he said “Lack of transparency is a huge political advantage. And basically, call it the stupidity of the American voter or whatever, but basically that was really, really critical for the thing to pass”.
Another leading Obama-era behaviorist who has also returned to power under Biden is Cass Sunstein (Obama’s regulatory czar) who wrote “once we know that people are human and have some Homer Simpson in them, then there’s a lot that can be done to manipulate them.”
The Liverpool Care Pathway (LCP) which Berwick wished to guide US health reform gives us another insight into the genocidal nature of this utilitarian approach to health services. According to Professor Pullicino, over 130,000 deaths/year were caused by the LCP which had gained influence over hospitals, hospices, nursing homes in the UK between 1995-2013. The LCP had essentially pressured thousands of healthcare providers to put millions of sick and elderly (and expensive) patients onto “End of Life” lists without their consent resulting in forced dehydration and morphine drips to accelerate deaths despite the fact that life-saving treatments were still available. The scandal caused by these revelations resulted in the LCP’s dissolution in 2014 although the Daily Telegraph pointed out that the program was merely rebranded and continues to this day.
Together, Berwick, Gruber and Emmanuel ensured that hospitals would be penalized for overtreating patients, and cancelled Medicaid coverage for swaths of cancer drugs and screenings for patients whose needs outpaced their QALYs. This logic may work when deciding to scrap an old car but creates severe moral dilemmas when applied to grandma.
You might now ask: But why must doctors abide by the demands of an independent board of cost-cutting experts? Why would doctors not simply reject the demands that abrogated their Hippocratic oaths and consciences?
With 2/3rd of all doctors beholden to other larger employers (vs the 85% of US physicians who were self-employed in 1963), the pressure to abide by rules of scarcity and cost-effectiveness mandates imposed by technocrats have grown immensely. As surgeries, cancer screenings and ambulatory services have been drastically cut under COVID protocols, hospitals which rely on government funding have suffered financially and have been losing $50 billion/month according to Rick Pollack (President of the American Hospital Association) who recently stated “I think it’s fair to say that hospitals are facing perhaps the greatest challenge that they have ever faced in their history.”
Euthanasia Across the Five Eyes
After decades of lobbying funded in large measure by George Soros’ Open Society Foundations globally, there are currently five nations which have completely legalized euthanasia (Canada, Belgium, the Netherlands, Germany and Columbia) while nine states in the USA have followed suite.
In Canada, euthanasia laws were first passed in 2016 with fairly strict restrictions requiring patients be terminally ill with a prognosis of six months or less while also being mentally sound directly before death is induced.
Yet, just after the US elections in 2020, and under the fog of COVID, Canadian House of Commons passed the Medical Assistance in Dying Act (Bill C7) which entirely removed all safeguards including requirements of a “reasonably foreseeable” death, long waiting periods and requirements of mental competency immediately prior to death.
Should the Senate pass the bill later this month as is currently expected, anyone suffering from depression (which has radically skyrocketed among the elderly and incapacitated locked in isolation from their friends and loved ones under months of COVID lockdown) may now request death at 9am in the morning and be killed by noon. The typical long waiting times that gave depressed people a chance to self-reflect is now long gone.
Similar euthanasia protocols have ramped up across Australia as several states and territories have seen assisted suicide protocols applied under COVID-19. Among them Tasmania has announced euthanasia will be legalized on March 5, 2021, and Queensland will bring the “service” online by May 2021. Victoria was the first state to usher in euthanasia in June 2019 and Western Australia’s euthanasia laws will take effect in mid-2021. In New Zealand, the last of the Five Eyes states under examination, the vote to legalize euthanasia occurred in October 2020 and will be implemented this summer.
Rather than allowing oneself to get sucked into the abyss of bioethical mind games surrounding medical assisted suicide, it is more useful to keep these following questions in mind:
WHY are medical resources so supposedly scarce among the most developed sectors of the world?
Why do nations in across the trans Atlantic face such shortages of hospitals, doctors, screening treatments?
Why do hospitals continuously find themselves closing their doors while per capita beds decrease with every year?[1]
Why do citizens tolerate trillions of dollars spent on never-ending regime change wars abroad and bailouts to Wall Street speculators while accepting the idea that money for healthcare is intrinsically limited?
Revisiting Hitler’s T4 Health Reforms
After the Nuremburg hearings saw 7 of the 23 Nazi doctors (including Dr. Guett) put to death for their role in Hitler’s Tiergarten Fier health reforms, Nuremburg counsel Dr. Leo Alexander wrote in 1949:
“Whatever proportions these crimes finally assumed, it became evident to all who investigated them that they had started from small beginnings. The beginnings at first were merely a subtle shift in emphasis in basic attitude, basic in the euthanasia movement, that there is such a thing as life not worthy to be lived. This attitude in its early stages concerned itself merely with the severely and chronically sick. Gradually, the sphere of those to be included in this category was enlarged to encompass the socially unproductive, the ideologically unwanted, the racially unwanted, then finally all non-Germans. But it is important to realize that the infinitely small wedged-in lever from which this entire trend of mind received its impetus was the attitude toward the non-rehabilitatable sick”
In his essay, Dr. Alexander described the growth of the euthanasia laws in fascist Germany as the concept “lives unworthy of life” was first introduced into health policy. Under the guidance of “expert panels”, the T4 health codes soon became a driving force of eugenics that saw 270,000 non-Jewish Germans killed starting with handicapped children and elderly before the policy was expanded to embrace Jews, Gypsies and other target “unfit” groups.
As investigative journalist Nancy Spannaus wrote in 2013:
“The implication was clear. However, Hitler did not give his general order for killing off the insane (and others) until the war began, and resources became even scarcer. The order was written by hand by Hitler in October 1939–and backdated by him to the first day of the war, in September. In preparing it, he had stated that he “considered it to be proper that the `life unworthy of life’ of severely mentally ill persons be eliminated by actions that bring about death.” In this way, “a certain saving in hospitals, doctors, and nursing personnel could be brought about.” The title of Hitler’s order was “The Destruction of Lives Unworthy of Life,” and the standard was, as the order said, that the patients “considered incurable according to the best available human judgment of their state of health, be accorded a mercy death.”
The fact that the organizations promoting the rise of this eugenics policy throughout Nazi Germany and North America included such powerhouses as the Rockefeller Foundation, the Wellcome Trust and the Human Sterilization League for Human Betterment (today renamed “Engender Health”) which have all taken leading roles in the World Health Organization over recent decades is more than a little concerning. The fact that these eugenics organizations simply re-branded themselves after WWII and are now implicated in modern RNA vaccine development alongside the Galton Institute (formerly British Eugenics Association), Oxford’s AstraZeneca, Pfizer and the Bill and Melinda Gates Foundation should give any serious thinker pause as we consider what patterns of history we are willing to tolerate repeating in our presently precarious age.
[1] In 1980, the USA had 5810 community hospitals spread across 3000 counties with 6 beds allocated per 1000 people (987,000 beds total for 227 million citizens). By 2013, total beds had fallen by 25% and 15% of the hospitals had disappeared resulting in 3 beds/1000 people despite the fact that the population had grown by 130 million.
The author can be reached at [email protected]
Copyright © Matthew J.L. Ehret
 Biden: Naked Socialism/Technocracy for America; The Great Land Theft A new chapter in the Energy Wars
Biden: Naked Socialism/Technocracy for America; The Great Land Theft A new chapter in the Energy Wars