

Medicine is built around memorizing foundational axioms from which all other medical decisions and policies are made and any dissenting perspective is relentlessly ridiculed—despite the fact these axioms aren’t always correct. In the case of vaccines, to sustain their market, they have been presented as both “safe and effective,” leading to doctors frequently assuming anyone vaccinated for a disease cannot catch it and that any injuries occurring immediately after vaccination are unrelated coincidence—resulting in a frequent failure by physicians to diagnose either of these.
 Miller’s Review ...
Best Price: $8.32
Buy New $14.48
(as of 04:45 UTC - Details)
Miller’s Review ...
Best Price: $8.32
Buy New $14.48
(as of 04:45 UTC - Details)

In turn, throughout my life, I have noticed more people than I can count (including groups of people) come down with the flu after they receive the flu vaccine. Whenever this is brought up in medical circles, the response typically is “correlation is not causation” and being lectured on the fact the injected influenza vaccine does not contain any live viruses so it can’t give you the flu.
More recently, I (and quite a few of my colleagues) noticed that this also happened with the COVID vaccine and more concerningly, we would come across cases where the person we knew not only got COVID but in some cases became severely ill, had to be hospitalized and then died. While this was understandably “denied,” I soon came across research from the adverse event reporting databases which showed that the two most common causes of death seen in association with the COVID-19 vaccines were heart issues (e.g., dying suddenly) and COVID-19, with the heart issues typically being clustering near the time of vaccination, while after a few weeks, the most commonly reported cause of death following a COVID-19 vaccine was…COVID-19.
Note: this is also shown in national trends of COVID-19 cases and deaths, as they tended to spike after vaccination campaigns were conducted.
Since I saw this so frequently, it left me wondering exactly what was happening.
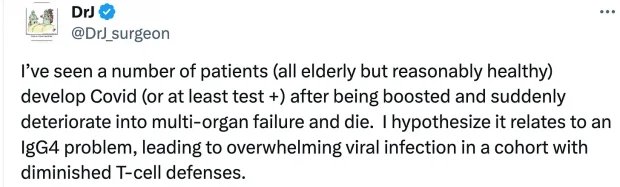
Note: one of the most convincing cases I saw came from a response submitted to a survey (Steve Kirsch had me analyze) where a man reported having a PCR confirmed (a-symptomatic) COVID-19 infection which immediately progressed to a severe infection after vaccination.
Initially, I suspected this was due to a hyper-inflammatory process. This was because many of the complications of COVID-19 are due to the immune system’s response to the virus rather than the virus itself (e.g., in hospitalized patients, as the disease progresses, the viral load often drops, but despite the virus being eliminated, the patients become more ill and the illness becomes more fibrotic in nature).
Note: one of the most interesting models I came across to treat COVID-19 came from Shankara Chetty, a South African doctor who concluded the body was forming an allergic response to the spike protein, which in turn necessitated either eliminating the virus early on (so this would not happen) or treating it as an allergy once the second phase began. Given that this worked for 7,000 people and his model matched what many of us observed, I found this theory quite compelling.
Since vaccines excessively stimulate the immune system, I theorized that the inflammatory response the vaccines create are tipping an already stressed system over the edge into a dangerous hyperinflammatory state.
Note: this is a common component of the Cell Danger Response, a chronic dysfunctional mitochondrial process which underlies many chronic conditions including chronic fatigue, long COVID and vaccine injuries.
This hypothesis in turn was reinforced by an inconvenient discovery with the HPV vaccine. For reference, the HPV vaccine was pushed upon the world under the theory that a chronic HPV infection could transform cervical tissue into cancerous tissue, and that since HPV was thus the cause of cervical cancer, preventing women from getting HPV through a vaccine could hence prevent women from getting cervical cancer.
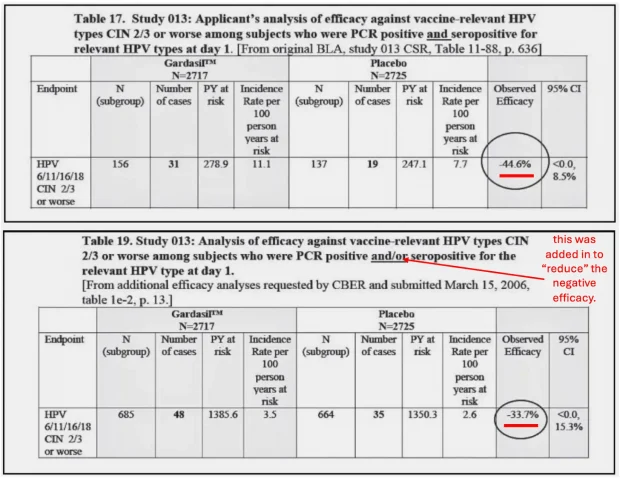
Unfortunately, there were a lot of holes in that chain of logic. One of these was the discovery that if someone was vaccinated for a strain of HPV they already had, it significantly increased their risk of getting cervical cancer.
Note: an identical effect was also found with GlaxoSmithKline’s competing HPV vaccine Cervarix. In a previous article on the subject of disease provocation, I took a deeper dive on the HPV vaccine provocation data and the other immense dangers of the vaccine.
However, requiring women to be tested for HPV prior to getting the vaccine would have significantly reduced vaccine sales (e.g., those who had already been infected wouldn’t vaccinate and many patients wouldn’t return for a follow-up visit once their negative test results had come in). This I believe explains why a decision was made to ignore this glaring problem and instead simply recommend beginning HPV vaccination at a much younger age (at 9-12) under the hope this would precede their first sexual exposure to the virus—which was unfortunate because the HPV vaccine had a very high rate of severe side effects, and it was not dosed at a lower amount for younger (and hence smaller) children.
Note: similarly, while individuals acutely ill with COVID were encouraged to wait a few days before vaccinating, the current guidelines do not advocate for having PCR test for COVID prior to vaccination (despite the fact so many were given that many Americans were receiving them on a weekly basis).
Like the COVID-19 example, I assumed “negative vaccine efficacy” had to be due to a hyperinflammatory response from vaccination (as the reason HPV created cervical cancer was due to the chronic inflammation it created in the cervical tissue).
Recently, as I began reviewing a remarkable collection of literature on the forgotten dangers of vaccination, I discovered that what I had observed with these vaccines was actually a longstanding problem that had been seen in the past with many other vaccinations, but sadly, again and again, that lesson was forgotten. Because of this data, I now believe this primary issue is not excessive inflammation but rather vaccine-induced immune suppression.
Note: a variety of mechanisms have been proposed to explain the significant immune suppression observed following COVID-19 vaccination (e.g., the COVID vaccine being shown to destroy of the hematopoietic stem cells which create a pivotal part of the immune system or antibody dependent enhancement—something known to observe with various vaccines including influenza and SARS). In this article I will primarily focus on one mechanism.
Original Antigenic Sin
Original Antigenic Sin (OAS) refers to the observation that if someone is vaccinated for a different strain than what is currently circulating (e.g., of the flu) they tend to have a worse immune response than those who were never vaccinated. Furthermore, multiple studies have shown that OAS affects completely different species (e.g., if you receive an influenza vaccine, you are less able to mount a response to “flus” caused by other respiratory viruses) and that OAS can persist for at least a year after vaccination.
 Anyone Who Tells You V...
Buy New $3.99
(as of 04:06 UTC - Details)
Anyone Who Tells You V...
Buy New $3.99
(as of 04:06 UTC - Details)
Note: in a previous article, I discussed a 2009 article, a 2009 study, a 2010 review, a 2010 study, and a 2013 study (published in peer-reviewed journals such as the Lancet), which collectively found a 40-166% increase in the likelihood of getting infected with a virus which differed from the strain you were vaccinated against (e.g., a pandemic influenza strain which had a greater risk of hospitalization) and up to a 100 fold increase in one’s viral load (which increases transmission). Additionally, in children who received a non-matching influenza vaccine, a 2012 study found they were 267% more likely to be hospitalized for influenza and another 2012 study found that 29.0% developed an infection with a non-influenza upper respiratory virus (compared to 3.4% of the unvaccinated). Finally, a 2023 study inadvertently showed influenza vaccination significantly increased one’s risk of being hospitalized for the flu.
OAS is thought to be a result of off-target immunity leading to partial immune suppression. Specifically, since the immune system has a finite ability to respond to threats, if it becomes hyper-primed to target one antigen (e.g., the vaccine antigen it is continually provoked to target), its focus is diverted away from other antigens it needs to respond to. This in turn makes sense since the immune system (which does not have an infinite number of immune cells) has to prioritize targeting life threatening infections, but unfortunately, since it did not evolve in tandem with the era of vaccination, it is not always prepared to appropriately to respond to the artificial immune stimulation vaccinations create.
Note: typically speaking, vaccine components persist in the body for a prolonged period (as the immune system cannot break down the immunostimulatory aluminum adjuvant they contain). This issue became a much greater problem with the COVID vaccines because the body has difficulty breaking down the synthetic mRNA they contain, which in many cases has led to the (immunostimulating) vaccine spike protein still being produced more than a year after vaccination.
In the case of influenza vaccinations, since the vaccines require months to produce and hence need to be made before the seasonal circulating strain is known, the wrong strain is frequently chosen. This leads to the annual vaccine often being ineffective, and worse still, frequently leading to OAS and exacerbating the existing flu season.
Note: in most “bad” influenza years, I typically hear colleagues argue that it’s a bad season because the wrong vaccine was chosen, but it’s still essential to vaccinate because had lots of people not vaccinated, that year’s flu would have been even worse (an effective marketing slogan which was repurposed throughout COVID). However, my own experience has been that whenever I saw someone in the ICU for an influenza infection during one of those “bad” seasons, their chart always showed they were vaccinated—an observation directly supported by some of the studies I linked to above.
Disease enhancement from a mismatching vaccine is a rarely discussed but well-known problem. For example, a reader and physician who worked in the NIH was assigned to study this issue from 2009-2011 and followed a cohort of vaccinated children and pregnant months over 3 flu seasons also discovered a clear trend of negative vaccine efficacy. When she submitted her analysis, however, she was removed from the NIH and blacklisted from future employment (and as a result, she understandably harbors great disdain for Anthony Fauci).
The solution Fauci and the NIH in turn pushed for was to utilize mRNA technology to produce seasonal influenza vaccines since the production time for them was much shorter (so they could begin being produced once the circulating flu strains were essentially known). Unfortunately, since SARS-CoV-2 mutated much faster than a typical influenza virus, even with this shortened production time, it was still not quick enough to match the circulating variants (even when now boosters were rolled out multiple times each year).
In turn, because of the focus over the last few years on studying everything related to COVID, a study of 51011 people at the Cleveland Clinic gave the most overt proof of OAS I have seen in the scientific literature as more vaccinations were directly correlated to one’s susceptibility to repeating COVID infections:
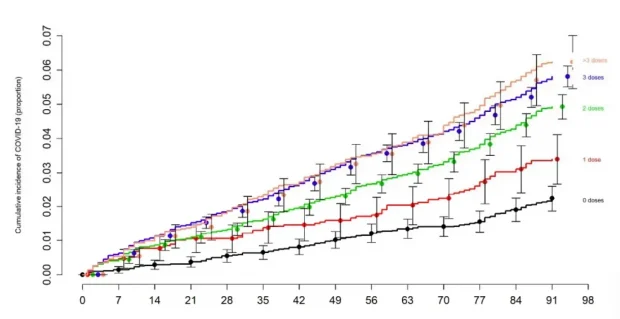
Note: there are many cases you can read online of individuals who have received multiple COVID boosters continually getting COVID (e.g., Igor Chudov periodically compiles them).
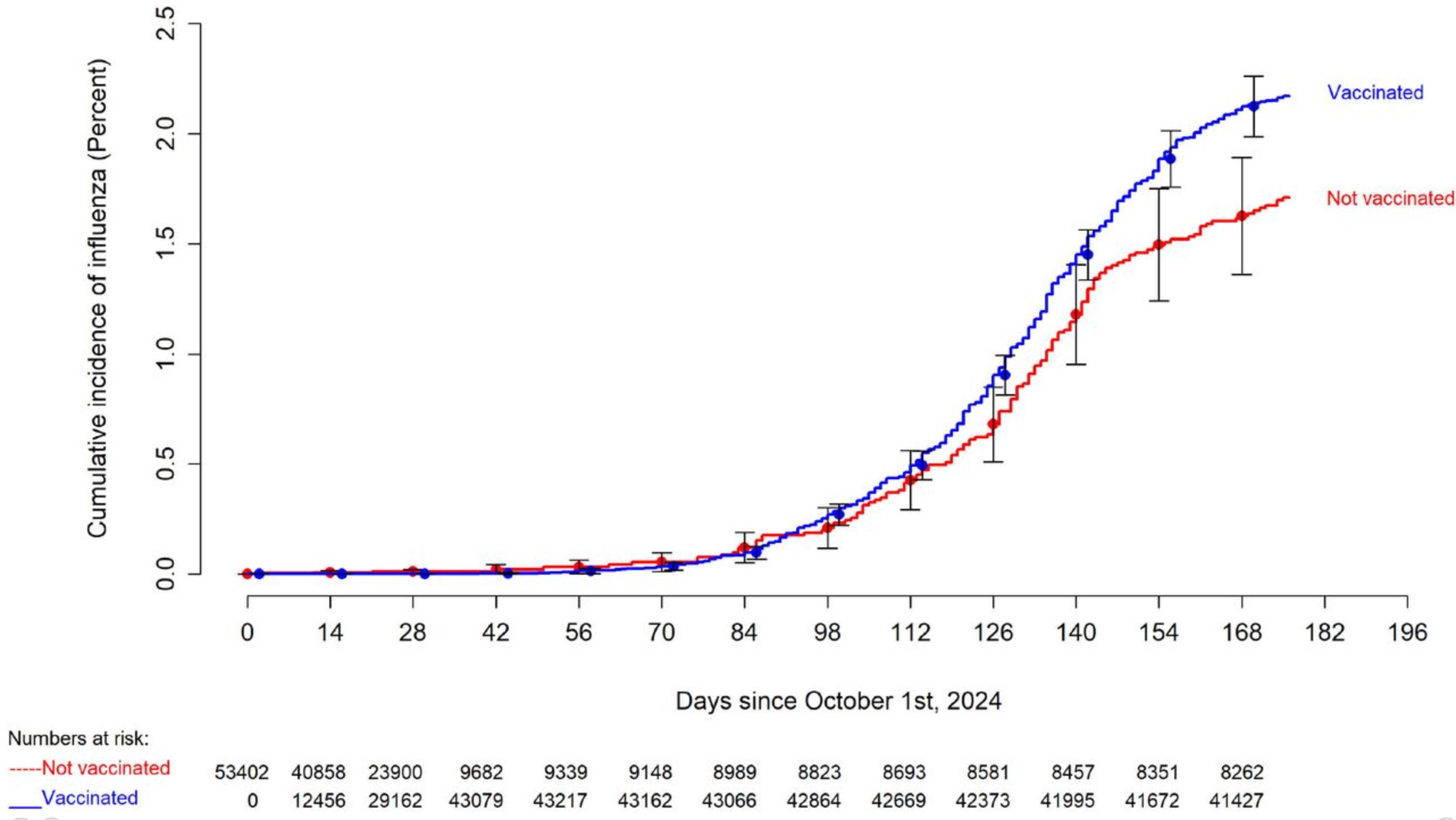
More recently, the Cleveland clinic published another dataset of 53,402 employees showing that the influenza vaccine actually increased ones likelihood of getting the flu.
One of the most tragic examples of OAS immunosuppression was Peter Aaby’s WHO studies which found childhood DTwP vaccination in Guinea-Bissau (a vaccine which is no longer used in the United States due to its toxicity) caused children to be 5 times more likely to die (3.93 for boys and 9.98 for girls)—something, which in most cases, was due to them succumbing from one of the many lethal infectious diseases circulating in Subsaharan Africa. Sadly, while his data was published, it was largely ignored by the global public health apparatus since it would have required abandoning a practice they were deeply invested in.

