



How Modern Medicine Made Your Bones Brittle
Why the drugs that raise your bone density often leave you more likely to break, and the forgotten ways to restore the strength of bone.
July 14, 2026
The years I have spent studying the medical industry have made me appreciate how often economic principles can allow one to understand its complex and contradictory behavior. For example, I believe many of the inconsistencies in medical ethics (e.g., “mothers have an absolute right to abort their children” and “mothers cannot refuse to vaccinate their children because it endangers their child’s life”) can be explained by simply acknowledging that whatever makes money is deemed “ethical.”
Sales Funnels
In my eyes, one of the most important business principles for understanding medicine are sales funnels, a method of selling products where you initially cast a wide net, and then successively cast smaller nets for increasingly expensive products after catching your initial customers.
Note: the term “funnels” is used to describe how the sales pipeline gets narrower as you move to more expensive products.
I typically see two types of (often overlapping) sales funnels in medicine.
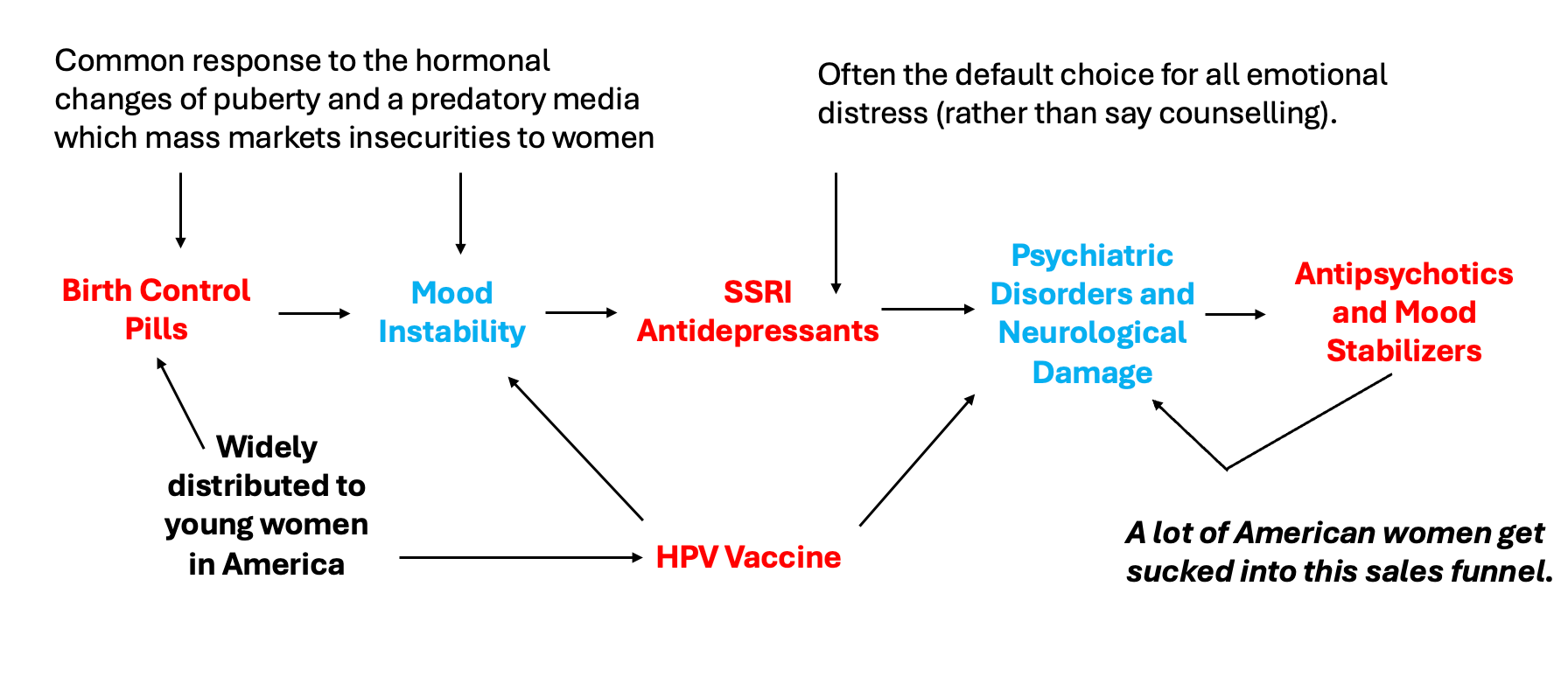
The first works by normalizing giving an “innocuous” drug to broad swathes of people and then selling increasingly expensive pharmaceutical drugs to treat the complications many experience from those drugs. One of the most insidious ones affects many of our girls and is one I’ve repeatedly tried to draw attention to:
Note: a good case can be made that many of the chronic illnesses our children suffer from now (which are very lucrative to “treat”) are a direct consequence of the ever increasing number of vaccines in the marketplace.
The second funnel works by recasting “preventative medicine” and “promoting health” as the task of screening for each person for conditions they are at risk for. The results from these universal screenings are then used to justify selling them medical services (e.g., drug prescriptions). Once that screening becomes normalized, the industry will then pivot to expanding the funnel and having far more services be sold. For example:
•What constitutes a “safe” blood pressure has been continually lowered, and as a result, more and more people are put on blood pressure medications. This in turn has created a variety of problems (discussed further here). For example, the elderly (due to the arteries calcifying with age) need a higher blood pressure for blood to reach the brain, and many hence suffer lightheadedness and catastrophic falls from their blood pressure being lowered.
•Since we started mass cholesterol screenings, what constitutes a “safe” cholesterol has also been continually lowered by the corrupt committees who create the guidelines doctors follow to practice medicine. For example, a widely used calculator which determines ones risk of a stroke or heart attack consistently concludes people are at a high risk of a heart attack and must urgently start statins, yet almost no doctor in practice knows that a 2016 study of 307,591 Americans discovered the calculator overestimates their risk by 5-6 times. Similarly, most doctors aren’t aware that beyond failing to benefit patients (in contrast to natural therapies which do improve heart disease), statins are also immensely dangerous drugs (discussed further here).
Note: the folly of this approach is highlighted by a trial which found removing on average 2.8 non-essential drugs from the elderly at one facility caused their 1 year death rate to go from 45%-21% and their hospitalizations that year to go from 30%-11.8%. As far as I know, there is no intervention on the market which offers a benefit comparable to this.
Radiographic Screenings
One of the common ways mass screenings are done is through giving lots of patients X-rays and then funneling those with abnormal imaging into being treated.
For example, women over the age of 50 are advised to get a mammogram every two years so that their deadly breast cancers can be identified and the women can be saved through early treatment for the cancers. However, whenever these screening programs are studied, they are found to not provide a net benefit because:
• Fast growing cancers (the ones you want to catch) will rarely be in the early stage at the exact same time someone gets a mammogram. Conversely, these cancers are normally noticed by doctors or patients (due to the sudden changes they create) and hence are radiographically evaluated independently of the mass screening programs.
• Slow growing cancers (which are unlikely to endanger women) are typically the ones which get caught.
• False positives are quite common with mammograms.
• A positive mammogram result is extremely psychologically stressful and frequently results in a variety of harmful treatments being performed on the women (e.g., having their breasts removed).
Peter Gøtzsche in turn conducted an exhaustive review of the evidence on routine mammogram screening which should have ended the practice (it can be read here). However, his data (which was widely publicized) had no effect on these screening programs. Many (myself included) believe that was because radiologists make so much money from mammograms they have an inherent need to justify the necessity of this routine screening.
Note: many medical specialists depend upon repeatedly performing the same billable service (e.g., vaccinating a child, performing a female pelvic exam, or reading a mammogram).
DEXA Scams
 Physician’s CHOI...
Check Amazon for Pricing.
Physician’s CHOI...
Check Amazon for Pricing.
 Another universal screening practice for women are dual energy X-ray absorptiometry (DEXA) scans, which calculate the density of bones and hence are believed to be a proxy for bone strength. It is then compared to the average bone density of a 30 year old, and a statistical method is applied to determine how far away their density is from that value which then produces their T-score. Every medical student in turn is taught that a T-score of 0 to -1 is normal, -1 to -2.5 is on the way to being bad (osteopenia) and a T-score that is -2.5 or worse means your bones are weak enough that you have osteoporosis and must urgently begin treatment for it.
Another universal screening practice for women are dual energy X-ray absorptiometry (DEXA) scans, which calculate the density of bones and hence are believed to be a proxy for bone strength. It is then compared to the average bone density of a 30 year old, and a statistical method is applied to determine how far away their density is from that value which then produces their T-score. Every medical student in turn is taught that a T-score of 0 to -1 is normal, -1 to -2.5 is on the way to being bad (osteopenia) and a T-score that is -2.5 or worse means your bones are weak enough that you have osteoporosis and must urgently begin treatment for it.
If you take a step back, a few questions should come to mind.
• First, since bones naturally become less dense with age, most people will have bones that are less dense than those of a 30 year old. In turn, the current management of osteoporosis accepts that bone loss is inevitable and reasonably tries to prevent that loss early on since it is so much harder to regain it later in life.
Hence, many people due to the normal process of aging will have osteopenia or osteoporosis. Consider for example what this study concluded was the average T-score by age of Italians.
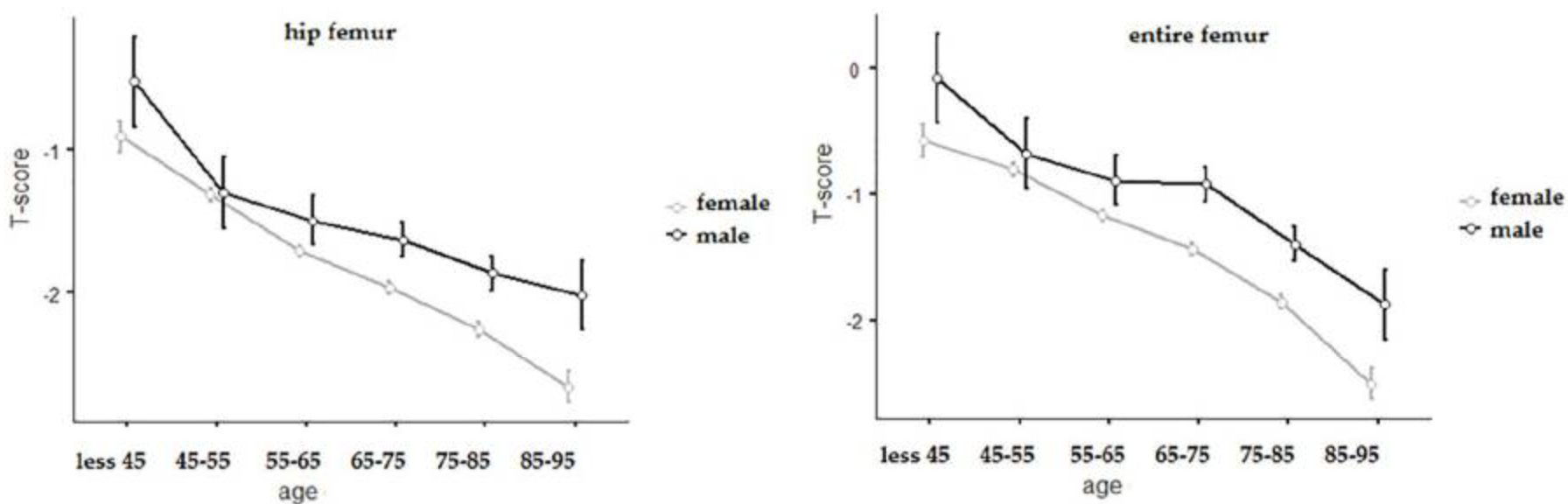
Note: if, for instance, the average T-score for a group is -2.5, this will mean a lot of people within that group (half of them) will have a score below -2.5 and conversely, at lower “averages” even more will have osteoporosis. Additionally, T-scores are calculated utilizing the standard deviation of the bone densities in 30 year olds, a value which can be up to 50% smaller than that of older adults (making it much easier to pass the -2.5 threshold). In contrast, a Z-score (which is not typically discussed or focused on) compares you to other people of your own age and sex and can tell you whether your bones are genuinely unusual for someone your age.
Where did this all come from? In 1994, a small WHO study group proposed that osteoporosis be diagnosed at 2.5 standard deviations below the mean of a healthy young adult, and osteopenia between 1.0 and 2.5 below it, hence classifying 52% of white women over 50 as having osteopenia and another 28% as having osteoporosis, leaving only 20% of them with “normal” bones. The authors themselves described their cut-off values as “somewhat arbitrary,” and the criteria were intended for epidemiological research rather than as the clinical treatment thresholds they immediately became.
 Magnesium Glycinate 40...
Check Amazon for Pricing.
Magnesium Glycinate 40...
Check Amazon for Pricing.
Note: as the BMJ later pointed out, the WHO report disclosed its own funding, and the disclosure reads: “This meeting was organized by the WHO Collaborating Centre for Metabolic Bone Disease, Sheffield, England, the World Health Organization and the European Foundation for Osteoporosis and Bone Disease, with financial support from the Rorer Foundation, Sandoz Pharmaceuticals and Smith Kline Beecham.” In short, the definition which converted 80% of older women into patients was written by a committee three pharmaceutical companies paid for (which is sadly a fairly common pattern—for example, absurdly low cholesterol thresholds are created by committees of doctors who were shown to be taking money from statin manufacturers) .
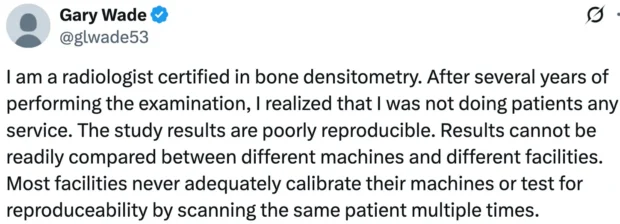
•Second, how accurate are the scans? As it turns out, there is actually a great deal of variance in DEXA scan results depending on which machine is used, how the operator performs the test and what bones are measured, with studies often finding a 5-6% difference in bone density depending on where the test was done. More importantly, since the T-score is based off standard deviations, a 5-6% difference in bone density can, in turn, change the T-score by 0.2-0.4 (which equates to a decade of bone loss) and hence tip many over to an osteoporosis diagnosis.
Note: a similar issue exists with blood pressure, as the stress of being a doctors office often creates enough of a BP elevation for people to be erroneously diagnosed with hypertension and started on blood pressure medications. This condition, in turn, is euphemistically known as “white coat hypertension,” applies to 15-30% of hypertension diagnoses, but rarely is corrected.
• Third, is there any point to repeatedly doing them? As it turns out, a study of 4124 older women found that once an initial DEXA result was obtained, there was no additional information of use gained from repeating the study over the next 8 years. Nonetheless, many guidelines often recommend getting a scan every 1-2 years, and likewise, Medicare pays for one every 2 years. As these scans typically cost between $150 to $300, that quickly adds up.
• Fourth, do the scans accurately reflect bone strength and the risk of fractures? While they are generally predictive of the risk, they are not as accurate as is commonly believed. For example, this study found the osteoporosis status of a patient (determined by their T-score) frequently did not match what was directly observed within bones under a microscope. Similarly, this study found that when bones were deliberately weakened, DEXA scans underestimated how much strength had been lost.
Furthermore, this is corroborated by publications in top journals:
 Naturebell Pure Magnes...
Check Amazon for Pricing.
Naturebell Pure Magnes...
Check Amazon for Pricing.
• One review estimated that roughly 85% of the contribution to fracture risk is unrelated to bone density altogether, and that over half of fragility fractures occur in people who cannot be classified as having osteoporosis at all.
• The 2019 paper “Two-Thirds of All Fractures Are Not Attributable to Osteoporosis and Advancing Age” followed 3,700 adults for decades and found that only 16% of fractures in women and 15% in men could be attributed to low bone density, and that nearly 73% of the women and 94% of the men who actually broke a bone did not have osteoporotic bone density on their scans.
• In 1996, the Swedish Council on Technology Assessment pooled eleven study populations encompassing roughly 90,000 person-years of observation and over 2,000 fractures to determine how well bone density predicts who will break a bone. Their conclusion, published in the BMJ, was that while bone density can predict fracture risk across a population, it “cannot identify individuals who will have a fracture,” and they stated plainly:
We do not recommend a programme of screening menopausal women for osteoporosis by measuring bone density.
In other words, medicine has known for years that the number it screens for, diagnoses with, medicates against, and re-scans every two years is not the number which determines whether your bones break. It simply has not changed anything, because that number is what the entire apparatus is built to sell.
 PreserVision AREDS 2 E...
Check Amazon for Pricing.
PreserVision AREDS 2 E...
Check Amazon for Pricing.
 Natureu2019s Bounty Zi...
Check Amazon for Pricing.
Natureu2019s Bounty Zi...
Check Amazon for Pricing.
 Nature Made Magnesium ...
Check Amazon for Pricing.
Nature Made Magnesium ...
Check Amazon for Pricing.
 Collagen Peptides Powd...
Buy New $27.95
(as of 10:50 UTC - Details)
Collagen Peptides Powd...
Buy New $27.95
(as of 10:50 UTC - Details)
Copyright © A Midwestern Doctor
 While the Political Circus Distracts Us, Flock Builds the Digital Police State
While the Political Circus Distracts Us, Flock Builds the Digital Police State