



How They Rig Clinical Trials and the Price We All Pay for It
A practical guide to spotting doctored research and finding the therapies that actually help
June 4, 2026
Every medical system in history has been great at addressing certain issues, so-so at others (requiring patients with those issues to see a highly talented practitioner for a successful resolution) and unable to address the rest. For this reason, I’ve long believed the “best” approach to practicing medicine is to develop an in-depth understanding of 1-3 medical systems, and then once you are aware of the therapeutic gaps in your tool box, recognize when another system has something which can address one of those gaps and fold that approaches into your framework.
In contrast, our society has been conditioned to believe that modern biomedical medicine is the one true system of medicine and that through a robust scientific process, has solved all the previous problems and mishaps which characterized its predecessors (so if any other modality wishes to be used in medical practice it must prove itself by the standards modern medicine has established). However, while that’s a nice-sounding idea, modern medicine is still bound to the same laws which dictate every other medical system, and as such, the reality in healthcare is:
• Conventional medical care is very good at addressing many issues, to the point we take for granted those issues are easily fixable (when for much of history they were not).
• Conventional medicine offers mediocre, less than satisfactory, or highly inconsistent results for many medical conditions large numbers of people suffer from along with proclaiming that for many illnesses “nothing can be done.”
• A variety of alternative therapies exist which can satisfactorily address many of the issues conventional medicine fails in, but rather than be embraced, they are widely disparaged as pseudoscience and quackery (which is why a thriving alternative medical field has persisted in the United States despite immense efforts to stamp it out).
To illustrate this point, I’ve focused on DMSO in this newsletter as it has a vast body of literature supporting its safe use for a myriad of challenging conditions. More importantly, due to how dramatic its efficacy is for many “incurable” conditions, I’ve now had thousands of readers submit (currently 6500) almost unbelievable testimonials showing DMSO rapidly cured their ailments (which I have been slowly compiling in articles specific to those ailments).
All of that raises an obvious question; how could a therapy like this remain completely unknown (particularly since in DMSO’s case, scientists, legislators and the public fought the FDA for decades for DMSO to be recognized), especially since the number one concern in healthcare for decades has been reining in its ever-increasing costs?
Note: the reason I continue to emphasize DMSO is that it has been one of the most efficient ways to meet the goals of this newsletter—helping people and providing clear proof of healthcare corruption. In practice, I use many other suppressed modalities that I would like to cover here, but as my time is limited and these articles take a lot of work to write, I have to prioritize where the effort will go the furthest rather than follow my personal interests (which will be covered in the future).
RCT Fundamentalism
In a recent article, I put forward the case that there is a very poor cost-to-benefit ratio from the existing clinical trial framework.
The current devotion to randomized controlled trials essentially resulted from:
- The FDA interpreting a 1962 Law (designed to prevent the next thalidomide) which stated The H.H.S. Secretary could block any drug from being marketed if it had a lack of “well-controlled investigations” to mean that no drug could be approved for use in the United States unless it had large randomized double-blind trials (RCTs) demonstrating its efficacy (excluding cases where the FDA felt like partially waiving that requirement).
- Reformers in the 1990s seeking to address medicine’s longstanding problem with dogmatic and counterproductive ideas persisting through replacing the existing status quo of deferring to experts with one where medical decisions should be dictated by “the best available evidence,” “individual clinical expertise” and “the patient’s unique values and circumstances.” Sadly, this was rapidly corrupted and switched to only prioritizing “the best available evidence” (e.g., vaccine mandates violate “patient values”) and “the best available evidence” being defined as evidence which met a statutory threshold (large RCTs and “expert” endorsement) rather than the best evidence currently existing on a topic.
Because of this, situations would frequently be encountered where it was clear there was an issue (e.g., a pharmaceutical or vaccine continually injuring someone) or something different needed to be done (e.g., DMSO being used for a debilitating, costly and incurable illness) but those alternative approaches would be blocked because there was no robust RCT supporting their use (and none would ever be done).
Note: DMSO is nearly impossible to conduct a blinded trial on because it produces immediate benefits no other therapy will produce, often causes brief skin irritation or a characteristic odor and will improve areas of the body besides where it was applied. As such, the FDA relentlessly insisted you could not claim the “non-blinded” trials demonstrating DMSO’s efficacy actually constituted proof it worked.
All of this, in turn, results from the fact RCTs have a few critical features most people are not aware of.
First, they are excellent at identifying small data signals which would be nearly impossible for individual practitioners to recognize (e.g., a 3% increase in the risk of a heart attack). This is extremely valuable when there is ambiguity in a routine clinical decision that is regularly made on a large basis each day (as those small differences rapidly add up) or for identifying serious rare side effects from a therapy. However, drug benefits detected in this manner often have very little relevance to routine medical care because they are so small most patients will experience no real benefit from those drugs (and hence why many patients have concluded its a waste of time to visit the doctor for most issues).
Second, while RCTs excel at evaluating pharmaceuticals delivered in standardized doses, they have a fundamental design mismatch with many non-drug therapies. These therapies are often highly individualized and context-dependent, heavily reliant on practitioner skill and the therapeutic alliance, difficult or impossible to blind effectively (with sham controls often proving non-inert), and capable of producing large, rapid, or multifaceted effects that do not align with the ‘small signal’ statistical methods RCTs are optimized to detect in large, homogeneous populations. Moreover, they often rest on holistic diagnostic frameworks and therapeutic philosophies that clash with the reductionist assumptions (and hence the patient allocation and stratification) of the RCT paradigm and success in these systems is frequently defined by outcomes (such as shifts in vitality) that cannot be meaningfully quantified or prioritized within the RCT model. As a result, promising therapies that fall outside the ‘one pill, one disease’ framework are perpetually marginalized, not necessarily because they lack efficacy, but because they cannot readily produce the specific form of evidence the RCT paradigm was designed to generate.
Third, the placebo effect, combined with the bias introduced when clinical trial observers know a patient is receiving treatment, will make a therapy appear more effective than it actually is. However, what most people do not know is that placebo effect is modest (giving an additional 30-60% improvement) and primarily seen in subjective symptoms (e.g., mood or pain) rather than objective biological shifts (e.g., blood sugar or a tumor size). Likewise, a detailed review found unblinded observers overestimate subjective patient improvements by roughly 36%. This means that while eliminating these biases with RCTs is helpful, it is not always essential.
Fourth, large RCTs are extremely expensive to conduct (typically in the tens of millions of dollars). This introduces three major problems:
•It is only possible for pharmaceutical companies, national governments, and massive NGOs (e.g., The Gates Foundation) to conduct them. Because of this, many topics which should be researched are simply “off-limits” and never researched (e.g., because the tiny amount of money which can be made from an off-patent does not justify a far more costly clinical trial or because they could produce results which threaten a profitable product).
• Because the clinical trials cost so much money to fund, it creates a natural incentive to doctor their results so that a positive outcome can be produced that justifies the massive investment which went into them.
• Because so much money exists in the clinical research field, so many people are invested in the current status quo that they will collectively defend its most egregious abuses while simultaneously reflexively attacking any competing model that challenges their authority over what constitutes valid evidence. Likewise, most biomedical researchers will not pursue controversial topics because producing results that challenge the status quo is economic suicide, cutting them off from the grants they depend on (a tactic Fauci weaponized to silence his critics and hijack science) or any opportunities for the other career path, pharmaceutical industry employment.
In addition to America having poor health outcomes despite vast spending on research and medical care (we spend by far the most but have the worst healthcare amongst the affluent nations), three data points directly dispel the value of RCT fundamentalism.
First, a definitive 2017 Cochrane review found that industry-sponsored drug studies were 34% more likely to report favorable overall conclusions than non-industry-sponsored studies.
Note: other studies have found higher percentages (e.g., 300%), but even at 34%, this means the bias effectively outweighs what these costly studies counteract by addressing the placebo effect.
Second, a definitive 2014 Cochrane Review found that smaller unblinded observational trials typically yielded the same results as large RCTs—which I suspect was due to the fact observational trials are typically only done when the magnitude of an effect is large enough for doctors to notice it (and hence for it to be clinically relevant). This is a critical review, as unlike large RCTs, smaller observational trials are affordable enough that anyone can conduct them, thereby making it possible to break the pharmaceutical industry’s monopolization of medical “truth.”
Note: institutional review processes that were designed to protect research subjects have increasingly become gatekeepers of orthodoxy, making it nearly impossible to obtain approval for even simple human studies on anything deemed controversial (which was incredibly frustrating for me and many others to deal with). This is why so much of the compelling research on therapies like DMSO comes from an era before these barriers existed or from countries where they still don’t.
Third, despite using the best tools science had to offer, spending far more than any other country, and imposing draconian health measures which have destroyed public trust in medicine, the US nonetheless had some of the worst COVID-19 outcomes.
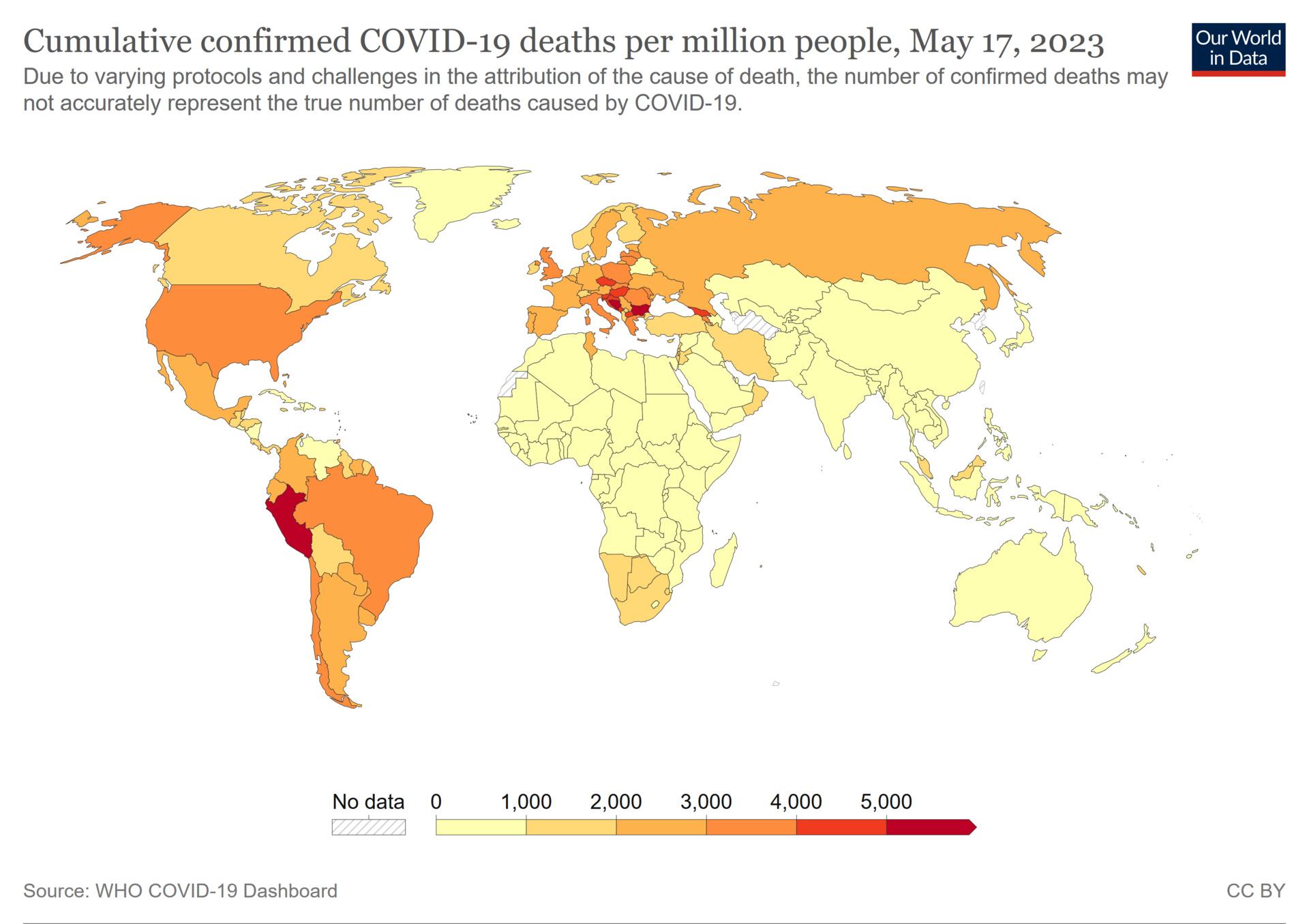
Put differently, many African countries which did virtually nothing for COVID (as they could not afford to) had between a 10-20 per million persons death rate from COVID, whereas the United States recorded 3,625 deaths per million and, beyond its standard medical expenditures, spent roughly $5 trillion in direct appropriations, plus far more in indirect costs from lockdowns and vaccine injuries, triggering a wave of inflation that reached approximately 30% over the last seven years, with housing prices surging 50-60%. This produced the greatest wealth transfer in history to the top 1%, hollowed out the middle class, priced an entire generation out of home ownership, and reduced daily life for millions of Americans into a struggle to simply get by.
That’s appalling, particularly since all of it could have been prevented if effective treatments had existed for COVID-19 (e.g., ICU doctors I spoke to in the early days of the pandemic who were being overloaded with COVID-19 all felt the single most important thing to do was create some type of viable early outpatient COVID-19 treatment). However, despite many effective treatments being developed (e.g., in my previous article, I highlighted the simplest and most widely available one, home upper airway disinfection) the standard of care remained “take Tylenol or Ibuprofen [which often made things worse] and come back to the hospital if you can’t breathe.”
Because of this, one group (c19early.org) collaborated to synthesize all the existing data on COVID-19 treatments so an alternative to the government guideline could be available. When I saw one of their charts synthesizing all the available COVID-19 research, a depressing pattern immediately jumped out to me, so I marked the chart up to highlight it:

Essentially, what this showed is that there was no correlation between a treatment’s efficacy and if it ended up in treatment guidelines. Rather, it was primarily a result of how profitable the therapy was (presumably because that propelled the lobbying necessary to get it approved), and more remarkably, the therapies developed by our robust clinical trial process were amongst the worst options available, which in part was due to the fact the committee which created America’s guidelines was selected by Fauci (who’d previously stonewalled every efficacious therapy for AIDS to push AZT through) and nearly everyone Fauci put on it had previously taken money from remdesivir’s manufacturer.
Note: in the previous article here, I documented how every year since 1976, the government has hyped a viral pandemic and has now funneled billions upon billions into proprietary countermeasures that failed—which has persisted because no one is ever held accountable for any of it. This year marks the fiftieth anniversary of that enterprise.
In short, RCTs are an incredibly useful tool for discerning truth, but the moment you rely upon them as the only tool for discerning truth and guiding clinical decisions, many medical problems will rapidly become unsolvable.
Copyright © A Midwestern Doctor
 Gitmo and Torture Revisited
Gitmo and Torture Revisited