



Understanding Blood Pressure in a Healthy Way
March 6, 2026
Ever since I first entered the medical field, something struck me as off about the relentless focus on blood pressure, and over time I noticed that the blood pressures people reported to me varied widely. While pondering this, a talented practitioner and mentor once told me that the current medical paradigm fixates on blood pressure because it’s easier to measure than blood perfusion (healthy blood flow).
Then, as I became more acquainted with the medical field, I began to notice a consistent pattern—whenever a drug existed that could treat a number or statistic, as the years went by, the acceptable number kept on being narrowed, making more and more people eligible to take the drugs that treated the number.
Conventional Blood Pressure Perspectives
 A Statin-Free Life
Check Amazon for Pricing.
A Statin-Free Life
Check Amazon for Pricing.
 Since blood vessels are elastic fluid-filled structures, that fluid holds them under pressure. Blood pressure, in turn, is typically measured by determining how much external force is needed to exceed the artery’s pressure and compress it so that blood no longer flows through it. Low blood pressure (hypotension) is a problem because it prevents blood from reaching the areas where it’s needed, but in most cases, medicine instead focuses on the consequences of high blood pressure.
Since blood vessels are elastic fluid-filled structures, that fluid holds them under pressure. Blood pressure, in turn, is typically measured by determining how much external force is needed to exceed the artery’s pressure and compress it so that blood no longer flows through it. Low blood pressure (hypotension) is a problem because it prevents blood from reaching the areas where it’s needed, but in most cases, medicine instead focuses on the consequences of high blood pressure.
Within the conventional model, those consequences are:
• Weakened blood vessels become more likely to break open and leak as higher blood pressure pushes against them. This for instance, is why Emergency Rooms aggressively lower the blood pressure of patients who show up with symptoms of “hypertensive emergency,” such as a severe headache and a significantly elevated blood pressure. Likewise, whenever a critical blood vessel ruptures (e.g., the aorta or one in the brain), once the bleed has been confirmed, the first step in managing it is to lower the patient’s blood pressure (so less blood leaks out) after which they are sent to surgery.
• Excessive pressure on the arteries strains and damages them, causing the lining of the vessels to become damaged and gradually develop atherosclerosis.
• Excessive blood pressure damages the internal organs (termed end-organ damage), leading to premature failure and early death (e.g., from a heart attack or kidney failure)—something which also results from chronic insufficient blood flow.
Because of this, high blood pressure is viewed as one of the leading preventable causes of cardiovascular disease; therefore, ensuring that a patient achieves sufficiently reduced blood pressure is a primary focus of all medical visits.
Unfortunately, that chain of logic has quite a few holes in it.
Variable Blood Pressure
Blood pressure (BP) is highly variable, especially at the periphery, where it’s typically measured. This variability—around 14 points—can lead to misdiagnoses of hypertension and unnecessary medication, which can lower BP too much, causing hypotension. One common form of this misdiagnosis is known as White Coat Hypertension, where the stress of visiting a doctor temporarily raises BP. This affects 15-30% of patients “diagnosed” with hypertension. Guidelines recommend confirming hypertension with multiple measurements, including home monitoring, but this is often not done.
 The Great Cholesterol ...
Check Amazon for Pricing.
Measurement errors, such as using the wrong cuff size or failing to account for differences in BP between arms, contribute to the issue. It’s estimated that 25% of hypertension diagnoses are incorrect. Moreover, there is often a poor correlation between peripheral BP (limbs) and central BP (inside the aorta). Central BP, which is more closely linked to cardiovascular disease, can differ significantly from arm readings. Different BP medications also affect central and peripheral BP differently, adding complexity to treatment.
The Great Cholesterol ...
Check Amazon for Pricing.
Measurement errors, such as using the wrong cuff size or failing to account for differences in BP between arms, contribute to the issue. It’s estimated that 25% of hypertension diagnoses are incorrect. Moreover, there is often a poor correlation between peripheral BP (limbs) and central BP (inside the aorta). Central BP, which is more closely linked to cardiovascular disease, can differ significantly from arm readings. Different BP medications also affect central and peripheral BP differently, adding complexity to treatment.
What Affects Blood Pressure?
If fluid at a set pressure tries to move through a tube, as the tube shrinks, the pressure it creates (e.g., on the walls of the tube) will increase, while if the tube enlarges, the pressure it exerts will decrease. The body continually controls where blood in the body goes by changing the heart rate and fully or partially constricting the arteries, allowing it to shunt blood to where it is most needed (e.g., by dilating arteries in that area).
Blood pressure is thus a product of two factors: the volume of blood in the arteries and the degree of arterial constriction or relaxation.
Note: since arterial BP is greater than venous BP, it’s what’s measured externally (as veins compress long before arteries do, and only arterial blood has a signature pulsatile wave created by the heartbeat).
Since each heartbeat pushes blood into the arteries and thereby increases the pressure within them, two blood pressure values exist—the baseline pressure (diastolic pressure, DBP) and the pressure when the heart contracts (systolic pressure, SBP). The blood pressure values you see (e.g., 140/90) represent the maximum and minimum.
Note: one reason why this stretching is important is that when the vessels contract back to their normal size once the systolic pressure fades, that recoil pushes blood further along into the circulation.
Blood pressure lowering medications in turn work by some combination of:
- Loosening the arterial walls
- Reducing the total blood in circulation
- Weakening the contraction of the heart
What Causes High Blood Pressure?
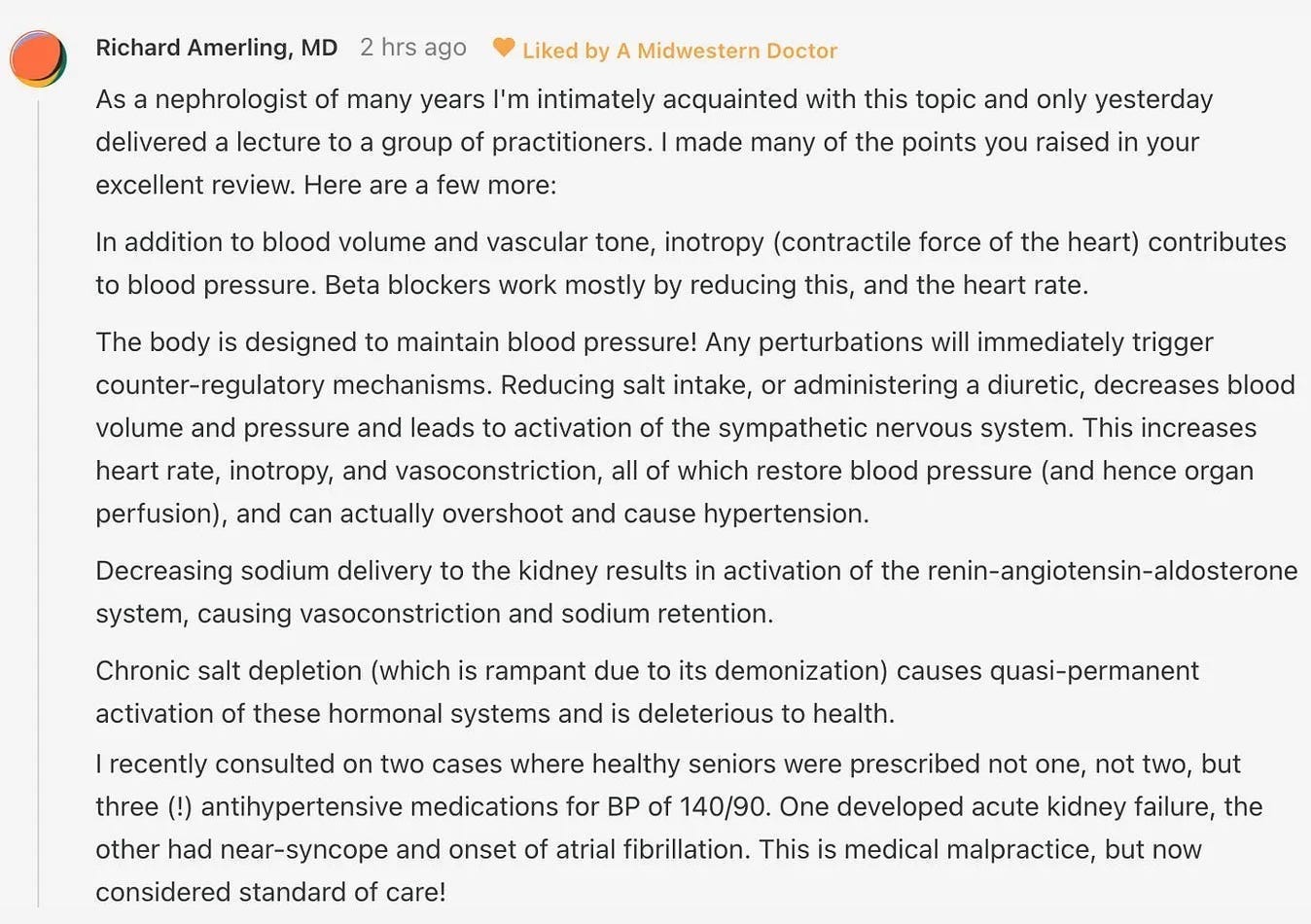
Most cases of high blood pressure (90-95% of them) are what is known as “essential hypertension” or “primary hypertension” which is a fancy (and rarely questioned) way of saying “elevated blood pressure without a known cause.” More importantly, the fact there is no known cause for most cases of elevated blood pressure has been a widespread belief in medicine for decades. Typically, the only cause we hear about is “not eating salt,” despite the fact that the most detailed review of this subject found that drastic salt reduction typically results in less than a 1% reduction in blood pressure and more importantly, that eating salt is actually critically important for health (discussed further here).
For the remaining 5-10% (known as secondary hypertension), recognized causes include reduced blood flow to the kidneys (which sets off a signal to raise the blood pressure because the kidneys believe there isn’t enough blood perfusion), sleep apnea, or having a rare tumor that releases a blood pressure increasing hormone).
 Vaccines, Amen: The Re...
Check Amazon for Pricing.
Vaccines, Amen: The Re...
Check Amazon for Pricing.
Since the cause of most hypertension is unclear, medicine simply focuses on risk factors like age, diabetes, salt intake, obesity, stress, and family history.
Note: effectively addressing anxiety can often cure high blood pressure that would otherwise be perpetually medicated.
Atherosclerosis and Blood Pressure
Many of my colleagues became suspicious of the traditional blood pressure model after observing that circulatory impairments often co-occurred with rising blood pressure rather than resulting from long-term damage. This led us to conclude that elevated blood pressure might be a compensatory response to inadequate blood flow, similar to how the kidneys raise blood pressure when they don’t receive enough blood.
Several factors support this idea:
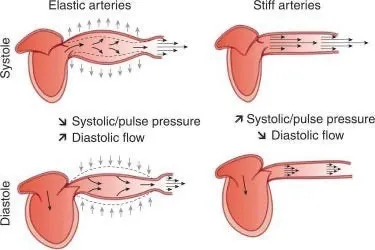
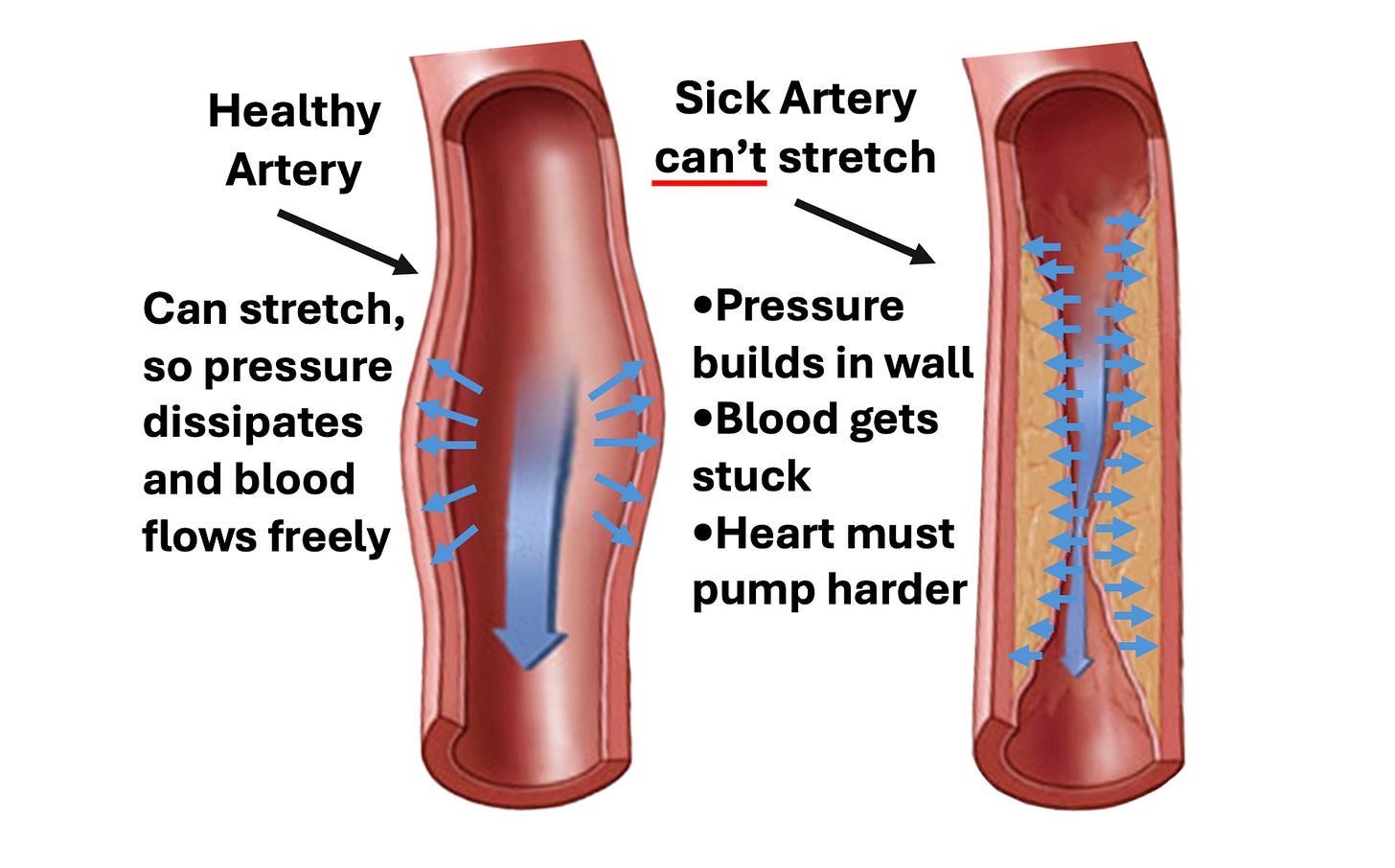
- Arterial Stiffening: Calcified arteries can’t expand as effectively, raising blood pressure as they become less able to release pressure.
- Measurement Inaccuracy: Blood pressure cuffs may overestimate pressure in stiffened arteries, particularly in those with severe atherosclerosis, resulting in higher readings than the true pressure (because hardened arteries require greater pressure to compress).
- Endothelial Dysfunction: The blood vessel lining releases nitric oxide to dilate vessels and decrease pressure. When this function fails, it precedes atherosclerosis and increases blood pressure, suggesting the problem is with endothelial health, not high blood pressure itself.
- Sympathetic Reflex: When the body rapidly loses a significant amount of blood, a reflex triggers increased heart rate and vessel constriction to raise blood pressure, a common response in critical conditions.
This all suggests that high blood pressure may be more of a symptom than the root cause of circulatory issues.
Note: as I show here, a strong case can also be made that the blood thickening and clumping together causes hypertension.
Changing Guidelines
When the blood pressure craze took off, there was a rush to bring the blood pressure lowering drugs to market before their benefit was actually proven (outside of a few short term studies which showed a small benefit for people with very high blood pressures).
That mindset cemented itself, and as the years went by, regardless of the evidence arguing against it), the blood pressure thresholds kept on getting lowered so more and more people could put on blood pressure lowering medications. Because of this, roughly 60 million American adults (23%) now take these drugs.
 Vaccines: Mythology, I...
Check Amazon for Pricing.
Vaccines: Mythology, I...
Check Amazon for Pricing.
However, excessively lowering blood pressure cuts blood flow to parts of the body that can’t function without sufficient blood flow. For example, blood pressure medications increase the risk of kidney disease,1,2 and suddenly passing out (from insufficient blood flow to the brain) is one of the most common side effects of blood pressure medications.1,2
My best guess is that this inexorable march to putting everyone on these drugs is due to some combination of the following:
• Research funding is available for these areas (e.g., from the drug manufacturers), hence being a safe area of research for academics to explore.
• It illustrates the “if you have a hammer, everything looks like a nail” phenomenon and the medical profession’s desire to find more justifications for using its tools (especially since humans tend to double down on their existing approach when it fails rather than consider a new one).
Let’s now look at how the blood pressure guidelines have changed over the years.
Note: as these guidelines show, originally the focus was on treating diastolic blood pressure under the belief that the heart had to “work harder” if there was too much blood in the circulation. I believe this is helpful to note since it was believed for decades (but now is not), and hence illustrates how arbitrary many medical dogmas are.
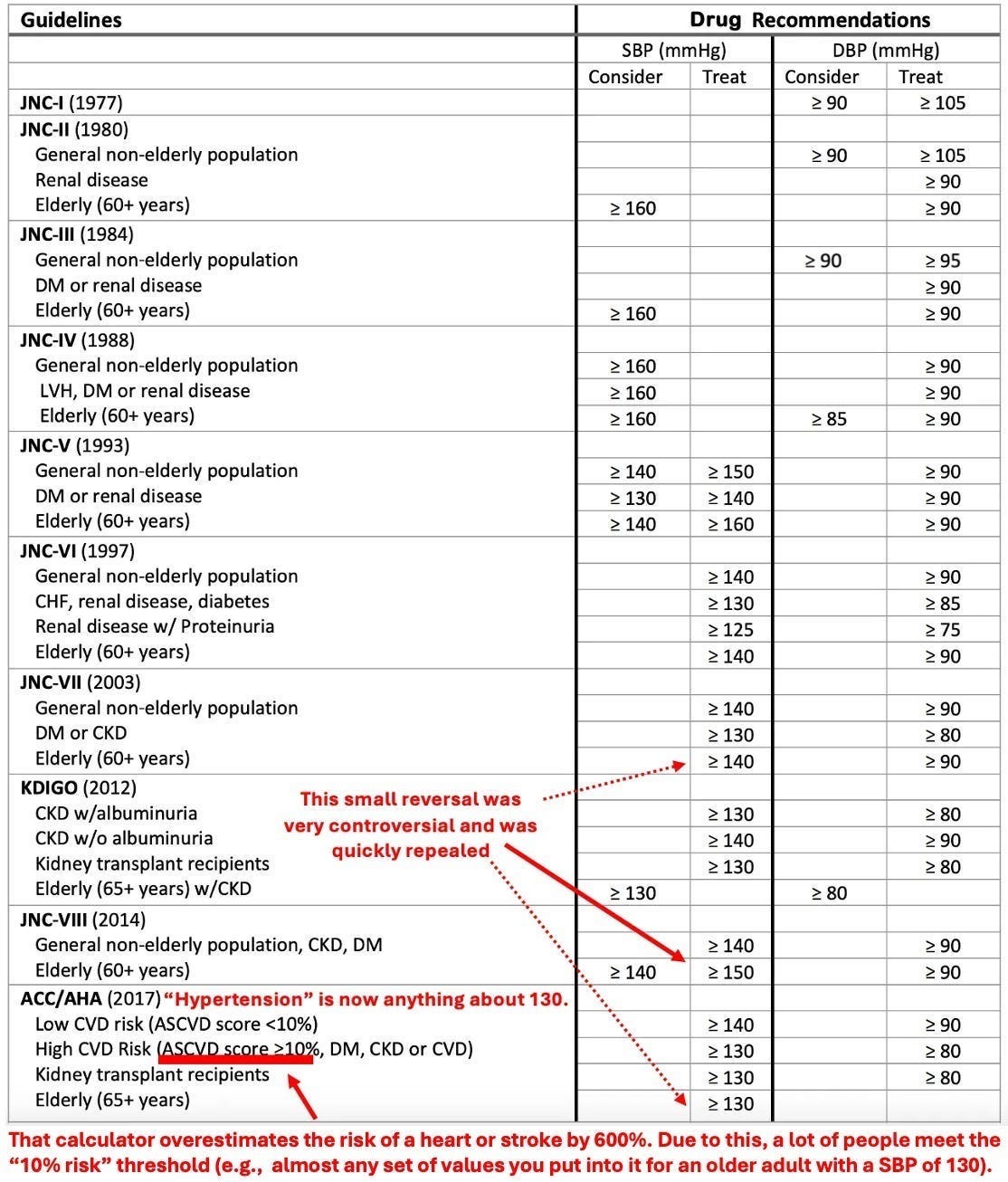
“Rather than 1 in 3 U.S. adults having high blood pressure (32 percent) with the previous definition, the new guidelines will result in nearly half of the U.S. adult population (46 percent) having high blood pressure, or hypertension.”
Note: this rate further increases with age (e.g., 79% of men and 85% of women over 75 now have hypertension, while 71% of men and 78% of women now meet the threshold to start blood pressure medications).
Unfortunately, “Experts” on guideline panels are paid to create recommendations that result in more and more people taking the drugs, a sadly common phenomenon in medicine. For example, once statins entered the market (which unlike their predecessors, could effectively lower cholesterol), the acceptable blood cholesterol levels kept on being lowered, and before long almost everyone was told they would die from a heart attack unless they started a statin—despite statins have an almost non-existing mortality benefit (e.g., taking them for five years at best makes you live 3-4 days longer) and causing (often severe) side effects for roughly 20% of users. In turn, since so many people have been severely harmed by the great statin scam, more and more people, such as comedian Jimmy Dore, have begun to speak out against this:
The Effects of Hypertensive Medications
In many cases, the actual mechanism of a drug greatly differs from the purported one (e.g., the tiny benefit statins provide is most likely due to them reducing inflammation).
 Dissolving Illusions: ...
Check Amazon for Pricing.
In the case of blood pressure medications (each of which works in a different manner), very different degrees of benefit are observed with their use, despite producing the same drop in blood pressure. This in turn strongly argues that their benefits are not due to them lowering blood pressure, but rather how each one specifically affects the body. To illustrate:
Dissolving Illusions: ...
Check Amazon for Pricing.
In the case of blood pressure medications (each of which works in a different manner), very different degrees of benefit are observed with their use, despite producing the same drop in blood pressure. This in turn strongly argues that their benefits are not due to them lowering blood pressure, but rather how each one specifically affects the body. To illustrate:
• A 1997 paper in JAMA reviewed the literature and found significantly different benefits from the antihypertensive drugs depending on which type was used.
• A 1998 review found that the (known) cardiovascular benefits of ACE inhibitors were not seen with calcium channel blockers, despite the latter having a more significant effect on blood pressure.
• A 2000 study of 3577 diabetics found that a specific ACE inhibitor, despite minimally reducing blood pressure (a 2.4 reduction in SBP and 1.0 reduction in DBP) had a massive effect (a 25% reduction) on the risk of a heart attack, stroke or cardiovascular death.
• A 2007, eight year long (and NIH funded) double-blind study of 42,418 subjects found that when two different types of blood pressure medications were used, there was no difference in their effect on blood pressure but simultaneously, found their rate of preventing heart failure varied by 18% to 80% depending on the drug, leading the investigations to conclude: “blood pressure reduction is an inadequate surrogate marker for health benefits in hypertension.”
 Amazon eGift Card - Ha...
Check Amazon for Pricing.
Amazon eGift Card - Ha...
Check Amazon for Pricing.
 Visa Physical Gift Car...
Check Amazon for Pricing.
Visa Physical Gift Car...
Check Amazon for Pricing.
 Roblox Digital Gift Ca...
Check Amazon for Pricing.
Roblox Digital Gift Ca...
Check Amazon for Pricing.
 $50 Visa Gift Card (pl...
Buy New $54.95
(as of 10:51 UTC - Details)
$50 Visa Gift Card (pl...
Buy New $54.95
(as of 10:51 UTC - Details)
Copyright © A Midwestern Doctor
 Dollar’s Debasement… Why Socialism Rises, and Wealth Taxes Follow
Dollar’s Debasement… Why Socialism Rises, and Wealth Taxes Follow