



The Hidden Dangers of Antidepressants and Why They're So Hard To Stop Taking
February 11, 2025
Whenever I ask a holistic physician which commonly used medication classes they believe cause the most harm to society, SSRIs always are one of the top five.
Note: statins (discussed here), NSAIDS like ibuprofen (discussed here), and PPI acid reflux medications (discussed here) frequently make the top five as well.
This is because SSRIs rarely benefit patients (only a minority of depressed patients have a metabolic type that responds to SSRIs) and the drugs have a large number of severe and often life-changing side effects. For example, in a survey of 1,829 patients on antidepressants in New Zealand:
• 62% reported sexual difficulties
• 60% felt emotionally numb
• 52% felt not like themselves
• 39% cared less about others
• 47% had experienced agitation
• 39% had experienced suicidal ideation.
Many of these can be immensely impactful for individuals (e.g., SSRI sexual dysfunction is often permanent and frequently causes severe depression, while emotional anesthesia takes away the joy of life and can cause people to spend years, if not decades, in emotionally toxic situations).
Worse still, the SSRIs are somewhat unique in that they can also harm those not taking the drugs as they can trigger psychotic violence, which results in either suicide, homicide, and tragically, in numerous cases, mass shootings (discussed further here). Furthermore, the pharmaceutical industry was aware of this from the start, but chose to conceal all that evidence to sell the drugs (and only revealed it after lawsuits forced them to).
Note: another example of a pharmaceutical that harms others is the COVID vaccine as it causes certain recipients to shed the vaccine and then significantly harm those around them who are sensitive to shedding—to the point numerous sensitive readers have shared COVID vaccine shedding has greatly impacted their lives (discussed further here).
Maximizing Sales
Much of the medical industry’s appalling conduct makes sense once its actions are viewed through a business lens that seeks to maximize sales. This for instance, is why the SSRIs, rather than being outlawed, were able to become some of the most successful drugs in history (e.g., in 2027, they are projected to be an 18.27 billion dollar global market) and why almost all of their appalling side effects have been hidden from the public. Let’s review some of those unconscionable tactics.
Sales Funnels
A classic principle in marketing is to cast as wide a net as possible for your customers and then gradually pull some of those customers into costlier and costlier products. Since funnels gradually shrink as you go further down them, similar to how fewer customers will buy a product as it becomes more expensive, this method is often referred to as a “sales funnel.”
With the SSRIs, a robust sales funnel exists as:
• Through years of almost unbelievable marketing (discussed further here), depression was redefined to include the normal negative emotions of life. As such, depression became so subjective it became possible to market it to most of the population and patients frequently will ask their doctors to prescribe SSRIs after they encounter an emotional obstacle.
• Numerous mass screening programs exist for doctors to diagnose if someone is depressed (e.g., this is routinely done for pregnant women and the elderly).
• Once a patient is “depressed,” rather than using natural approaches that effectively treat depression, the medical system will aggressively push them to start SSRIs.
• The SSRIs frequently cause a variety of psychiatric issues which require taking even stronger psychiatric medications.
Bipolar Disorder: An Unintended Outcome
Since the SSRIs antidepressants are stimulants, they often trigger mania. In turn, one of the most common problems associated with their use is bipolar disorder (a disease where you alternate from a depressed to a manic state). To put this into context, in 1955, 1 in 13,000 people were disabled for bipolar, and the majority of patients who presented to the hospital for a manic episode permanently recovered. Now, bipolar affects 1 in every 20-50 people, and 83% of them are severely impaired in some facet of their lives.
A significant amount of data has linked bipolar disorder to SSRIs. For example:
• Yale researchers reviewed the records of 87,290 patients diagnosed with depression or anxiety between 1997 and 2001 and determined those treated with antidepressants converted to bipolar at the rate of 7.7 percent per year (three times greater than the rate for those not exposed to the drugs), ultimately resulting in between 20-40% of depressed patients becoming bipolar.
• A survey found 60% of bipolar patients only developed their illness after receiving SSRIs for depression.
• Peter Breggin reported that of 184 patients in the hospital starting Prozac, Zoloft, or Paxil, 11 developed mania and 8 became psychotic, and in Yale, 8% of 533 consecutive admissions were for mania or psychosis caused by antidepressants, and two patients heard voices commanding them to kill themselves.
Note: the psychiatric field gets around this issue by claiming SSRIs “unmask” latent bipolar a patient always had—even though it likely would have never been “unmasked” had they never taken the SSRI in the first place.
Likewise, since the advent of mass psychiatric medicating, the character of bipolar has changed, becoming much more complicated to treat, characterized by much more rapid cycling between the depressed and manic states, and much more likely to produce severe complications like dementia later on. Unfortunately, when the foremost experts in bipolar disorder presented these findings at the American Psychiatric Association’s annual conference and urged caution in the over administration of SSRIs, they were met with boos from their increasingly upset audience.
As such, the link between SSRIs and bipolar disorder is rarely focused on, and instead the dangers of bipolar disorder (e.g., being 4-6 times as likely to die prematurely) are continually emphasized to justify treating it. This is remarkable given that a strong case can be made that many of the disastrous complications of bipolar disorder result from the highly toxic antipsychotics the disorder is “treated” with, especially since those same drugs are often given to schizophrenic patients, a disorder characterized by similar long term complications (that are rarely seen in countries which do not use the drugs).
In short, a robust sales funnel exists to create lifelong psychiatric medication users, best demonstrated by the fact spending an ever increasing amount of money to “treat” mental illness has only resulted more of it:
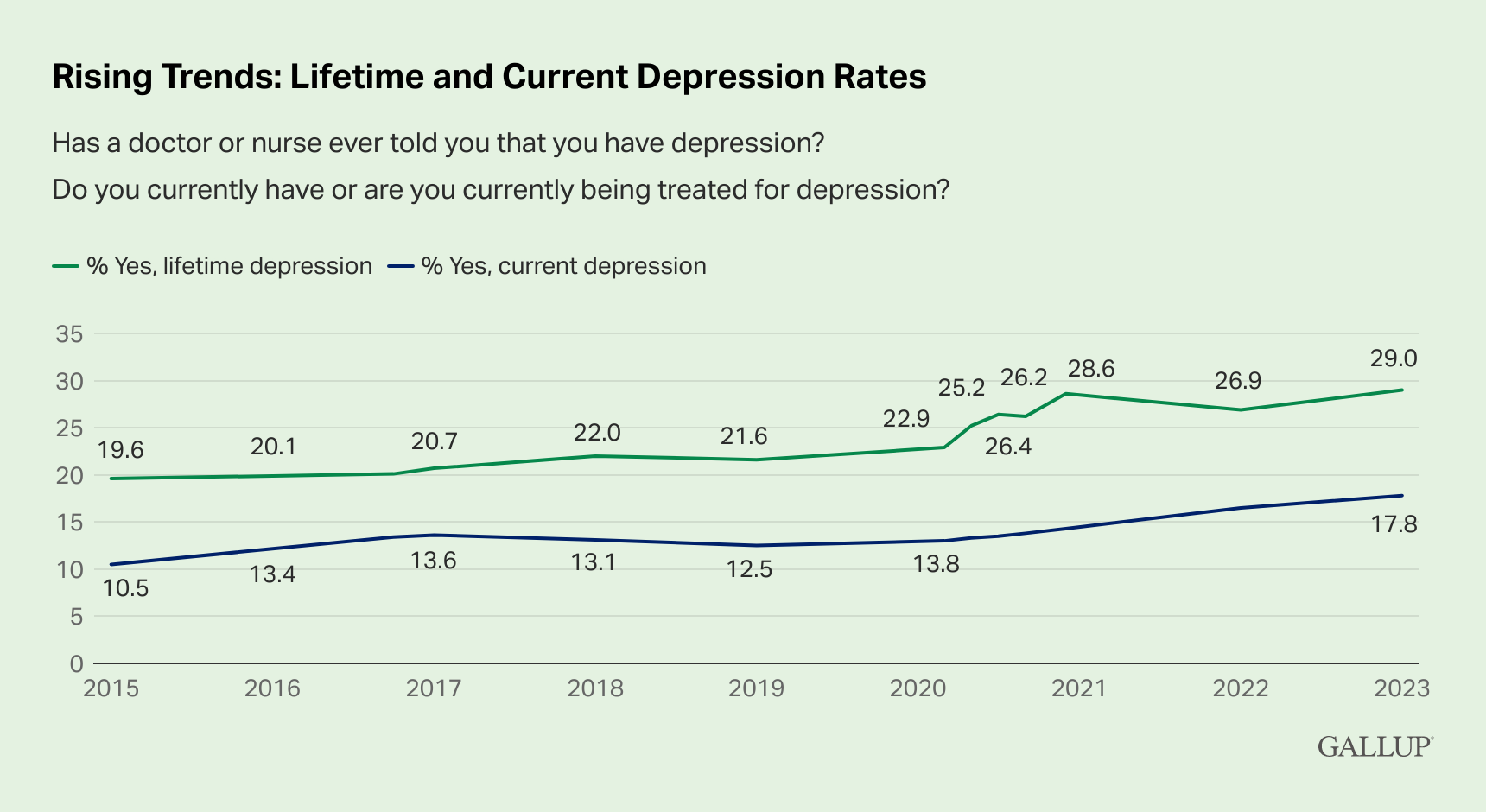
Worse still, this sales funnel is particularly effective in capturing young adults who were raised in it (e.g., a recent post-COVID survey of those aged 18-24 found 42% had a mental health condition, including 37.8% with anxiety and 32.8% depression)—and is particularly predatory towards young women:
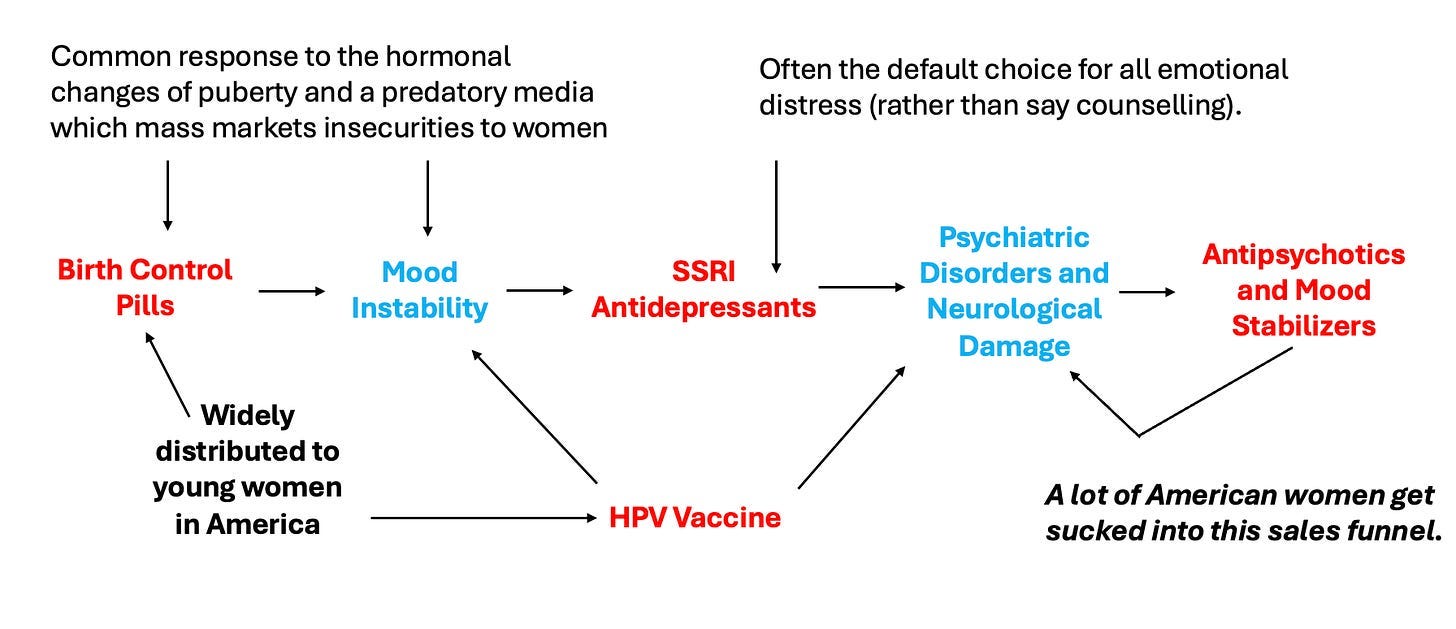
Note: birth control pills have been strongly linked to causing a variety of mood disorders and personality changes, including roughly doubling the likelihood of depression, with the greatest increase being seen in adolescent girls (a 130% increase). Given that 19.5% of adolescent American girls are put on the pill, those sales quickly add up.
Customer Retention
Since SSRIs “treat” rather than “cure” depression, they typically are a lifelong prescription (which is great for sales). However, since SSRIs have so many intolerable side effects and rarely help those who use them, tactics need to be used to retain those customers and safeguard their recurring revenue.
For instance, patients will often be told (sometimes not only by a doctor but also by a judge) that they lack the judgment to understand their mental illness, and they must hence take the prescribed medication. Likewise, physicians rarely recognize the adverse effects of SSRIs. Instead, they are often trained to attribute them to the patient’s pre-existing mental illness (which frequently leads to horrendous gaslighting and patients sometimes being forced to take the medications against their consent).
SSRI Withdrawals
Like many other stimulants, SSRIs can be extremely addictive. In fact, SSRIs have such a high risk for withdrawals that merely changing an existing dosage or accidentally missing a pill can be sufficient to trigger severe withdrawals (e.g., this has caused many SSRI suicides).
Unfortunately, when this happens, rather than recognize that withdrawals are occurring, physicians typically interpret them to mean the SSRI was effectively treating a severe (pre-existing) mental illness—and thus must urgently be resumed, even though the “mental illness” the patient exhibits was not present prior to them initiating the SSRI.
Likewise, since so few physicians know how to recognize the signs of SSRI withdrawals, almost none know how to treat it. As a result, individuals experiencing SSRI withdrawals frequently make the horrifying discovery that the safety net they thought existed simply isn’t there (an experience which likewise has been shared by many of those who developed significant complications from the COVID-19 vaccines).
As such, many who experience these withdrawals are forced to resume the drugs (as this is often all doctors can offer those patients), thereby ensuring customer retention.
Effects of SSRI Withdrawals
When withdrawing from an SSRI, severe withdrawals (e.g., becoming suicidal or violently psychotic) can happen. As such, I always urge readers to be extremely cautious in how they stop the medications.
However, far more frequently, less severe (and often fluctuating) withdrawal symptoms also occur such as:
• The feeling of an electric shock in your arms, legs, or head (these horrible things are commonly referred to as “brain zaps.”
• Dizziness (mild to severe)
• Visual problems
• Many sensitivities (e.g., to light, heat, a supplement or food).
• Anxiety, which comes and goes, sometimes in intense ‘surges’
• Difficulty in getting to sleep and vivid or frightening dreams
• Low mood, feeling unable to be interested in or enjoy things
• A sense of being physically unwell
• Rapidly changing moods (e.g., spontaneous weeping spells, attacks of sheer terror, or sudden plunges into unprecedented contentless black holes of pure dread).
• Anger, sleeplessness, tiredness, loss of coordination and headache
• A feeling that things are not real (‘derealisation’), or a feeling that you have ‘cotton wool in your head’
• Difficulty in concentrating
• Suicidal thoughts
• Queasiness or indigestion
• A feeling of inner restlessness and inability to stay still (this is known as akathisia and often precedes psychotic SSRI violence).
• Crippling muscle pain or spasms.
Worse still, these reactions are very common (e.g., I know more people than I can count who’ve experienced brain zaps).
In fact, a recent meta-analysis found that 56% of patients who stop using SSRIs experience withdrawals, that 46% who stop an SSRI experience severe withdrawals, and that these withdrawals last for weeks to months. Additionally, it is well known in the SSRI recovery community that the risk of a withdrawal varies greatly depending on the drug (e.g., Paxil is notorious for causing withdrawals, Cymbalta is also a common offender).
Note: a 1996 door-to-door survey of 2003 randomly selected people in England found that 78% of them considered SSRIs to be addictive.
The pharmaceutical industry is well aware of this, to the point they will often deliberately put “placebo” subjects in SSRI trials into withdrawals (by terminating their existing prescription) so they can make the drug group look “better” than the “placebo” patients or provide benzodiazepines to mitigate the negative side effects of the SSRIs (and hence remove them from the trial data).
Note: this is similar to how Merck hid Gardasil’s high rates of severe adverse reactions by using its toxic adjuvant (rather than saline) for the placebo group, resulting in similar injury rates in both groups, which, despite being extraordinarily high, went unquestioned by regulators.
Copyright © A Midwestern Doctor
 The US Should Not Take Over Gaza
The US Should Not Take Over Gaza