



Vaxx-Free Passports - The More Logical Measure
September 6, 2022
The government’s narrative about the unvaccinated is as accurate as the story about the unpopular kid having “cooties” that circulates on school playgrounds. On December 16, 2021, Joe Biden told the world that the unvaccinated were looking at a “winter of severe illness and death” and that getting vaccinated was the only real protection from the Omicron variant. He was replaying the tired, old narrative that the unvaccinated are sickly and put others at risk. In fact, the opposite of this is closer to the truth.
There’s growing evidence that the unvaccinated have fared better against COVID-19 than the vaccinated and that the vaccinated are more likely than the unvaccinated to spread SARS-CoV-2. This should come as no surprise to the well-informed because, even prior to COVID-19, evidence was mounting that many vaccines pose more risk than benefit. For example, research has found that children who are not vaccinated with the childhood vaccines, or only partially vaccinated with them, have better health outcomes than fully vaccinated children. Jeremy R. Hammond has reviewed some of this research in his article entitled “Oregon Medical Board Suspends Dr. Paul Thomas for Practicing Informed Consent” and his book entitled The War on Informed Consent.
The notion being pushed that safety requires the public to show proof of vaccination to move about, so called vaccine passports, is also reality turned on its head. In fact, safety would be furthered more by requiring proof of not having received certain vaccines—vaxx-free passports so to speak (i.e., swiping to electronically execute an affidavit swearing that one has not received a specific vaccine within some period of time, such as the last 30 days).
To be clear, this article is not advocating for the imposition of vaxx-free passport requirements, and especially not by government. Rather, it seeks to demonstrate that the consequences of vaccine use are far more complex than the public realizes and that many vaccines pose risks that extend beyond their recipients. Hopefully, business owners will come to understand these complexities, and the other side of the equation, and refuse to impose any type of vaccination proof requirements for entry into their establishments.
Depending on the type, vaccines can pose short-term and/or long-term societal risks.
Some vaccines pose an imminent risk to society, by creating the potential for vaccinees to transmit infectious agents to others. Several examples are discussed in the next section, below.
Some vaccines pose a long-term risk to society, by negatively impacting the course of infectious agents. Examples of these include strain resistance (e.g., vaccination for whooping cough, vaccination for measles); strain replacement with more dangerous strains (e.g., vaccination for HPV); increases in the incidence of one disease by vaccinating for another one (e.g., vaccination for chickenpox negatively affecting shingles); shifts in the pattern of infection to a more dangerous one (e.g., vaccination for measles); and interference with natural herd immunity (e.g., vaccination for measles). To use a crude analogy, the long-term societal impact of certain vaccines is akin to that of antibiotic use causing antibiotic resistance and exposing all to stronger bacteria.
Many vaccines can pose the risk of transmitting infectious agents to others.
Some vaccines used for the following diseases contain live attenuated viruses (LAVs): chickenpox, influenza, measles, mumps, rubella, polio, smallpox, monkeypox, rotavirus and yellow fever. As noted in a 2010 article discussing the development of LAV vaccines, “Because LAVs are shed from vaccinees, they sometimes present a risk to unvaccinated individuals with impaired immunity.”
Chickenpox Vaccination
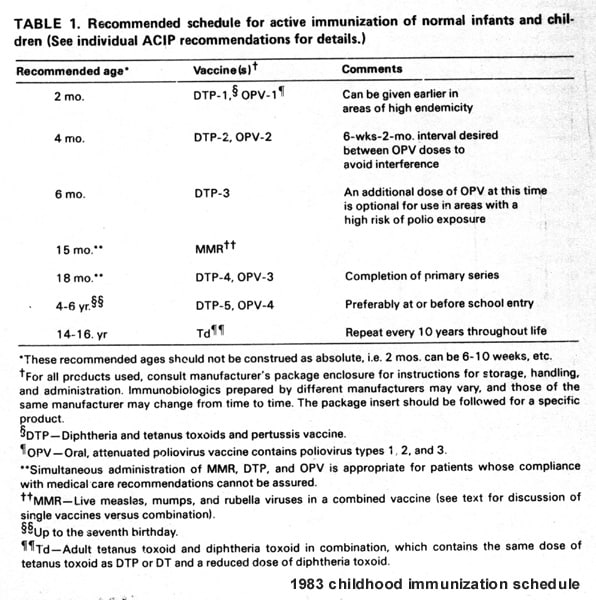
Since 1986, broad legal immunity has been granted to the manufacturers of vaccines recommended by the CDC for use in children, and this liability shield extends to the use of such vaccines in adults. Since then, the number of doses and vaccines on the CDC’s childhood schedule has increased alarmingly. In 1983, the CDC recommended 24 doses of 7 vaccines by age 18. The CDC currently recommends approximately 72 doses through age 18—up to 27 doses of 10 vaccines (14 antigens) through 15 months of age, another 13 doses of 8 vaccines (11 antigens) through age 18, plus one to two annual flu shot doses. Furthermore, one receiving all of the recommended doses on both the CDC’s childhood and adult schedules would receive approximately 150 doses.
The CDC recommends vaccination against chickenpox for both children and adults. It recommends the Varivax vaccine for this purpose, for both groups. Varivax is made from live, attenuated varicella virus and its package insert states:
Post-marketing experience suggests that transmission of varicella vaccine virus (Oka/Merck) resulting in varicella infection including disseminated disease may occur between vaccine recipients (who develop or do not develop a varicella-like rash) and contacts susceptible to varicella including healthy as well as high-risk individuals. Due to the concern for transmission of vaccine virus, vaccine recipients should attempt to avoid whenever possible close association with susceptible high-risk individuals for up to six weeks following vaccination with VARIVAX.
The CDC also recommends the use of the ProQuad vaccine against chickenpox for children, which is also made from live, attenuated varicella virus. It’s a “combination vaccine” used for measles, mumps, rubella, and chickenpox. The ProQuad package insert also contains warnings for vaccinees to avoid close contact with high-risk individuals susceptible to varicella and acknowledges that this should be done because transmissions of varicella vaccine virus may occur between vaccinees and the latter group.
Influenza Vaccination
The CDC recommends annual vaccination against influenza for both children and adults.
However, the CDC acknowledges that shedding can occur in connection with live attenuated influenza vaccine (LAIV). Discussion on the CDC’s website regarding LAIV states, “Shedding of the live attenuated vaccine virus is common after receipt of LAIV. In general, shedding is more common among younger recipients, among whom it may also be of longer duration.”
FluMist Quadrivalent is a LAIV recommended by the CDC for use in children and adults. Its package insert states, “17.2 Vaccination with a Live Virus Vaccine Inform vaccine recipients or their parents/guardians that FluMist Quadrivalent is an attenuated live virus vaccine and has the potential for transmission to immunocompromised household contacts.”
Measles Vaccination
Vaccination against measles is recommended by the CDC for both children and adults. The CDC recommends vaccines which contain live attenuated measles virus: M-M-R II and ProQuad.
Shedding can occur in connection with the use of measles vaccines using live attenuated measles virus. For example, in a 1995 study that examined the urine of children administered such vaccines, it was found that 83% (10 of 12) of the 15-month-old children studied had measles virus RNA in their urine for up to 14 days after vaccination. (The researchers only checked through day 14.)
Monkeypox Vaccination
Vaccinia infection is caused by infection with the vaccinia virus and monkeypox is caused by infection with the monkeypox virus. Both viruses are from the poxvirus family, genus Orthopoxvirus. Infection with orthopoxviruses can lead to localized or generalized skin lesions which progress from papules to vesicles and scabs and other symptoms such as fever, swollen lymph nodes, malaise, and body aches.
ACAM2000 is FDA approved for use against smallpox but has recently been made available for use in the U.S. against monkeypox under an expanded access application. (Prior to this, it was primarily used in the U.S. military for smallpox, but only on select, designated groups.)
The ACAM2000 package insert discusses the risks the vaccine poses for transmitting vaccinia virus, stating in part,
Patients must be advised that virus is shed from the cutaneous lesion at the site of inoculation from approximately Day 3 until scabbing occurs, typically between Days 14-21 after primary vaccination. Vaccinia virus may be transmitted by direct physical contact. Accidental infection of skin at sites other than the site of intentional vaccination (self-inoculation) may occur by trauma or scratching. Contact spread may also result in accidental inoculation of household members or other close contacts.
Two well-credentialed professionals from John Hopkins Center for Health Security, an epidemiologist and an infectious disease physician, recently expressed concern in an opinion piece about the risk of transmission posed by using ACAM2000 for monkeypox.
Polio Vaccination
In July of 2022, a case of polio was found in the state of New York. Of course, the unvaccinated were widely blamed for this on social media. Ironically, the case was caused by vaccine-derived poliovirus, not wild-strain poliovirus. In fact, as discussed in an article by Dr. Xiaoxu Sean Lin and Health 1+1 entitled “Polio: Why Vaccines Are to Blame for Rising Number of Cases”, polio is reemerging in many parts of the world due to use of oral poliovirus vaccines (OPVs), which use live attenuated poliovirus strains.
OPVs are not used in the U.S., where vaccines based on inactivated poliovirus are used. Nonetheless, people in other parts of the world who have been administered OPVs can and do make their way to the U.S. This is illustrated by a 2008 instance noted on the CDC’s webpage in which a Minnesota woman with vaccine-derived polio isolated from her stool developed paralytic polio and later died of polio-associated complications. It was determined that she was likely infected about 12 years prior to onset when her child received an OPV.
Conclusion
Although Joe Biden has warned Americans about the fairy tale risks of not receiving COVID-19 vaccines, he hasn’t warned them about evidence that those vaccines can cause serious harm. He also hasn’t warned them about risks posed by other vaccines being administered to Americans. With the pharmaceutical industry heavily influencing U.S. health policy, it’s not surprising that Biden sounds like a pharmaceutical vaccine rep, albeit a senile one.
The public is in dire need of education, not only about the risk of adverse reactions vaccines can pose, but also about the risk of transmission they can pose. In particular, the vaccinated among us in the habit of disparaging “anti-vaxxers” require enlightenment about the glass houses they’ve been living in as they’ve thrown their stones. Once the public more fully grasps the full consequences of vaccine use, hopefully we can all meet in the middle, vaxxed and unvaxxed, and agree to simply leave each other alone to manage our own health as we see fit.
Copyright © Davis Taylor
 The Booster Fanatics Aren't Giving Up
The Booster Fanatics Aren't Giving Up
{kind=link}