


Summer 2020 comes. The coronavirus cycle, which runs from November to April, follows the Summer solstice where the northern hemisphere tilts back towards the sun, and the resultant increased solar UV intensity increases sunshine vitamin D levels among those Americans who brave the outdoors in the midst of lockdown orders. That should normally quell the winter cold season till next fall.
The common cold coronavirus cycle runs from December through the end of April.

But just as laboratory confirmed cases of COVID-19 coronavirus decline, they suddenly rise. Here it is, early July, and Florida reportedly experiences the largest increase in cases of any State, 15,299 on a Sunday, July 12.

CDC changes the way it tabulates cases
The news media doesn’t inform the public the Centers for Disease Control has changed the way it determines COVID-19 severity and now includes symptomatic and asymptomatic cases in its tabulations. It is a categorical increase, not an increase in the spread or virility of the virus.
 Jillmo Bartender Trave...
Buy New $74.99
(as of 04:07 UTC - Details)
Jillmo Bartender Trave...
Buy New $74.99
(as of 04:07 UTC - Details)

The Center for Evidence-Based Medicine cites a broad range (5% to 80%) of people who test positive for COVID-19 but are without symptoms. This has led public health authorities to issue misdirected advisories to stay indoors as asymptomatic individuals may be spreading the virus. Everybody is then an imagined threat to your life. But it takes 40,500 encounters with infected people to get infected and over 6 million encounters to produce 1 death. Mask-wearing Americans are just mindlessly following devious instructions they hear on TV.
To-màto, to-mäto: infection/immunity
Of course, any viral infection has a Janus face, with infection increasing the percent of the population that develops antibodies and immunity. To confound matters, investigators find COVID-19 antibodies are not long-lasting and that zinc-dependent T-cells (produced in the thymus gland) actually halt the infection, which means immunity rates (~30%) are far higher than antibody tests have shown.
Antibody tests only reveal past infection. The commonly used polymerase chain reaction test (PCR), usually obtained via a mouth swab, indicates active infection. The problem with these tests is that they don’t point to any corrective therapy. A vitamin D blood test would. The American people are being conned.
TB OR COVID-19?
Tuberculosis is a bacterial lung infection with similar symptoms to COVID-19 coronavirus. It appears TB cases are intentionally being misclassified as COVID-19. COVID-19 responds to the same drugs used to treat TB (azithromycin, hydroxychloroquine). The BCG TB vaccination lowers the risk for COVID-19. TB outbreaks are where COVID-19s deaths have been reported.
A very revealing study conducted in the Philippines was recently published. Among 309 healthcare workers, 7 were diagnosed with COVID-19 coronavirus. Three (3) of these COVID-19 cases were among healthcare workers on the TB ward. So, forty (40) healthcare workers working on the TB ward and 26 TB patients who had come in contact with the three healthcare workers with a positive COVID-19 test and had respiratory symptoms were tested by PCR (polymerase chain reaction), and all were negative for COVID-19 coronavirus. All of the tested TB patients had TB and not COVID-19! None of the 40 healthcare workers had COVID-19 (except the original three). TB-coinfection may increase COVID-19 infection and mortality.
Deliberate misdirection?
 How Not To Die With Tr...
Best Price: $18.23
Buy New $17.97
(as of 08:00 UTC - Details)
It appears health authorities want to keep the masses vulnerable so they will beg for a vaccine that may or may not appear later in the year. Public health authorities need to conduct vitamin D tests on individuals who have remained indoors and compare with them with people who brave the outdoors.
How Not To Die With Tr...
Best Price: $18.23
Buy New $17.97
(as of 08:00 UTC - Details)
It appears health authorities want to keep the masses vulnerable so they will beg for a vaccine that may or may not appear later in the year. Public health authorities need to conduct vitamin D tests on individuals who have remained indoors and compare with them with people who brave the outdoors.
How to compare country data
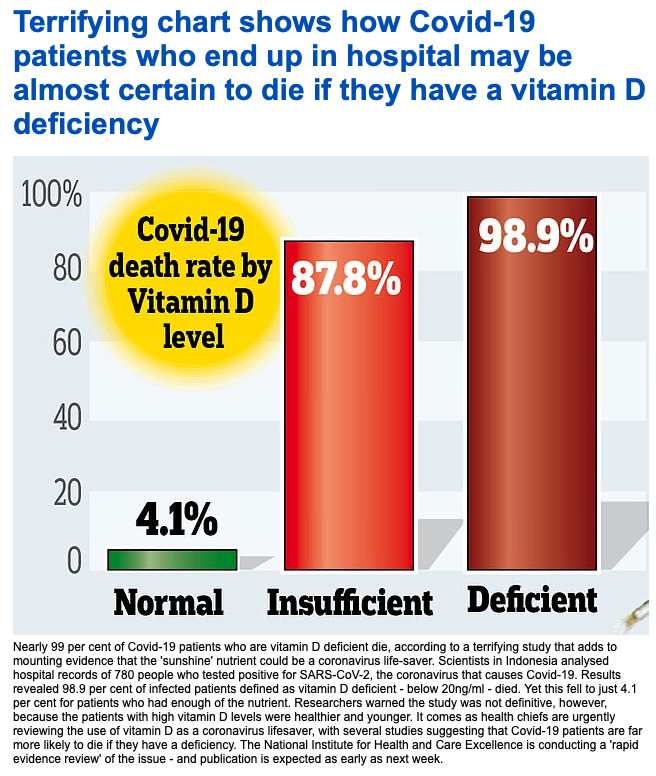
The current calculated number of laboratory-confirmed cases that worsen to the point of death (case/fatality rate) ranges from lows of 0.03% in Taiwan, 0.78% in Japan, to 14.4% in Italy, 15.4% in the UK, compared to 4.1% in the US.
Countries with low case-to-fatality rate like Chile, 2.2%; Peru 3.6%, Paraguay 0.7%, Venezuela 0.9%, are in the Southern Hemisphere and are just now entering their coronavirus cycle calendar-wise. So, their data is not comparable.
Some of the COVID-19 related deaths in countries like the US and Italy may be explained by large sub-populations of dark-skinned people (Liberian immigrants Italy; US blacks) and large populations of frail elderly subjects who largely live indoors who are more vulnerable to infection (large fraction of the population with co-morbidities) due to low vitamin D blood levels.
But unless a population-wide study is being done these tests would only serve to spread undue panic and fear.
Population at-large studies
Unless a population study is conducted of people that represent the community at large, testing is misleading. Such a population study was conducted in Santa Clara, California by Stanford and University of Southern California researchers and found 2.49 to 4.16% of the population tested positive for current or past COVID-19 coronavirus. The increases in cases (infections) you read or hear about in the news only reflects the intensity of testing.
According to the Centers for Disease Control, as of July 10, 2020, 40,787,857 tests have been done in the U.S., 3,663,490 (9%) which were positive for COVID-19. That figure includes false positives. This number (9%) is considerably higher than the study mentioned above (2.49-4.16%).
The public hears a lot about testing for COVID-19. Americans first heard the tests were in short supply. Then they heard the tests themselves were quarantined for faulty performance. Then news reports said there weren’t enough tests being done.
 Carleen White Gold Pla...
Buy New $19.99
(as of 04:07 UTC - Details)
Carleen White Gold Pla...
Buy New $19.99
(as of 04:07 UTC - Details)
The only plausible explanation is that more COVID-19 testing is being conducted since deaths are in decline, to drum up more fear.
What is the point of testing?
Answer: to strategically identify demographic groups, be it by location (hospitals, nursing homes, schools) or age (nursing homes, schools), or skin color (blacks), or by personal health habits (smoking, alcohol abuse) or by infirmity (diabetics, hypertensives, obese, autoimmune) that may be at higher risk for infection. That would reveal what strategic isolation, lockdown or quarantine measures need to be put into practice in order to limit the number of deaths and minimize the financial destruction caused by needless quarantine. At no time has this been done in the U.S.
Strict lock-down would be required to slow infection rates
Limiting the number of people infected is total impractical as very restrictive lockdown and quarantine measures would be required. At no time has the U.S. accomplished strict lockdown as the public has been allowed to go to grocery stores, drug stores, hospitals.
The main objective should be to limit COVID-19 associated deaths, not cases. Given COVID-19 infection induces mild-to-no symptoms, and infection produces antibodies that may serve prevent re-infection and further spread of the virus, prevention of cases is counterproductive.

South Korea’s remarkable success
South Korea has accomplished a remarkable feat. Just look at the chart below. Testing may have had something to do with keeping the COVID-19 mortality rates low, but precisely what? Tests aren’t medicine, unless it can be claimed there is some sort of placebo effect or that those who are tested maybe commonly do something to prevent death like take vitamin C pills.
Testing allows health authorities to quickly seal off high-risk groups from further contact with the outside world. South Korea found grade schools weren’t a hot spot for cases, so no efforts were made to close the schools. Nursing homes and healthcare workers inside clinics and emergency rooms where suspected COVID-19 patients were being examined were hot spots of COVID-19 cases. Special measures were taken to keep these high-risk areas in quarantine, practicing hand washing and other measures to prevent infection and spread.
Unlike the U.S., South Korea accomplished this without destroying their whole economy. South Korea started by trying to flatten the curve (keep hospitals from being overwhelmed) and ended up flat-lining deaths. Strategic measures paid off, as a report in the New York Times indicated.
But in the U.S., serious errors were made by politicians managing this epidemic. It seems as if these were by intent.
 MW Polar Peppered Smok...
Buy New $41.00 ($0.48 / Ounce)
(as of 04:07 UTC - Details)
MW Polar Peppered Smok...
Buy New $41.00 ($0.48 / Ounce)
(as of 04:07 UTC - Details)
The World Health Organization handbook for managing epidemics forbids politicians from attempting to gain popularity by grand-standing themselves in these situations. Health authorities should be the public spokespersons during these epidemics.
Governors of States shuttled infected patients into nursing homes by force of law, thus exposing frail, vulnerable institutionalized patients to this killer virus.
Politics over people; the political blame game
Scrap any idea modern medicine exists outside politics. Most of the COVID-19-related deaths emanate from States of the same political party. With an upcoming Presidential election, the excessive number of reported deaths in Democrat-controlled States is disconcerting. There are 24 Democrat governors and 26 Republican. Two-thirds of the cases are on the BLUE Democrat side. Six BLUE states have half the cases but only a third of the population.
U.S. politicians are bragging about the volume of tests performed but saying nothing about the failure to use these tests to target treatment and prevention towards high-risk groups and thus unlock the rest of the population and the economy from very destructive confinement.
Public health authorities should have:
- Forbidden admissions to nursing homes of COVID-19-infected patients transferred from hospitals.
- Mandated vitamin D testing upon admission to hospitals and conducted vitamin D testing on all nursing home residents and staff, given that adequate vitamin D levels drastically reduce COVID-19 related deaths. Ditto vitamin D testing for hospital staff. Recognize 42% of COVID-19 related deaths have occurred in nursing homes.
- Issued special precautionary bulletins to black American communities (churches, etc.) of their vulnerability and need for vitamin D testing and supplementation. Vitamin D pills should have been distributed from churches to the community for free. Black Americans are dying at three times the rate of white people.
The CDC admits “positive” COVID-19 blood tests may only indicate having a prior coronavirus “common cold”; and the CDC is mixing tests for the virus with tests conducted for antibodies to come up with a highly inflated number of cases.
We now have identified the high-risk groups. We don’t need testing. The tests are highly inaccurate anyway. They are unreliable. People are voluntarily confining themselves to their home when all the test indicated is that they had a coronavirus infection at some time in the distant past.
U.S. health authorities have already identified high-risk groups. There is no need for testing other than to help confirm a diagnosis, and no single test should be used for that purpose says a spokesperson for the American Lung Association.
Widespread testing is just being used now to create more fear-evoking news headlines. The masses are compliantly wearing masks and distancing for peace of mind only. Businesses are being crushed unjustifiably.

